

Equitable utilisation of Indian community based health insurance scheme among its rural membership: cluster randomised controlled trial
- PMID: 17526594
- PMCID: PMC1895633
- DOI: 10.1136/bmj.39192.719583.AE
Equitable utilisation of Indian community based health insurance scheme among its rural membership: cluster randomised controlled trial
Abstract
Objective: To evaluate alternative strategies for improving the uptake of benefits of a community based health insurance scheme by its poorest members.
Design: Prospective cluster randomised controlled trial.
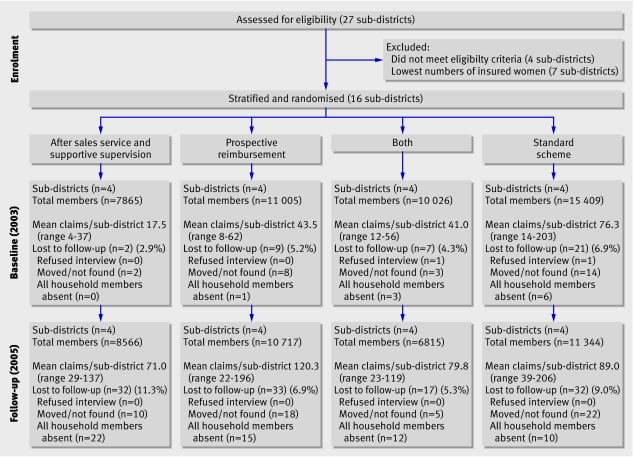
Setting: Self Employed Women's Association (SEWA) community based health insurance scheme in rural India. Participants 713 claimants at baseline (2003) and 1440 claimants two years later among scheme members in 16 rural sub-districts.
Interventions: After sales service with supportive supervision, prospective reimbursement, both packages, and neither package, randomised by sub-district.
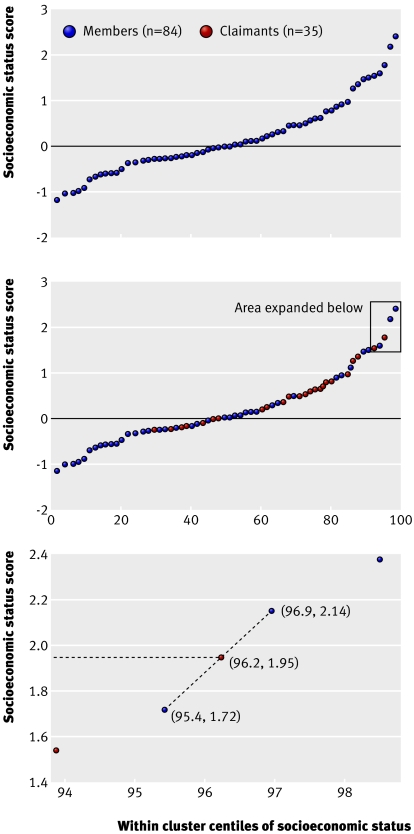
Main outcome measures: The primary outcome was socioeconomic status of claimants relative to members living in the same sub-district. Secondary outcomes were enrolment rates in SEWA Insurance, mean socioeconomic status of the insured population relative to the general rural population, and rate of claim submission.
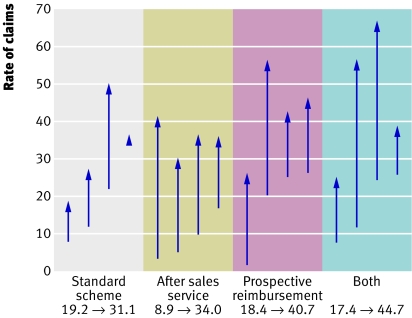
Results: Between 2003 and 2005, the mean socioeconomic status of SEWA Insurance members (relative to the rural population of Gujarat) increased significantly. Rates of claims also increased significantly, on average by 21.6 per 1000 members (P<0.001). However, differences between the intervention groups and the standard scheme were not significant. No systematic effect of time or interventions on the socioeconomic status of claimants relative to members in the same sub-district was found.
Conclusions: Neither intervention was sufficient to ensure that the poorer members in each sub-district were able to enjoy the greater share of the scheme benefits. Claim submission increased as a result of interventions that seem to have strengthened awareness of and trust in a community based health insurance scheme. Trial registration Clinical trials NCT00421629.
Trial registration: ClinicalTrials.gov NCT00421659.
Conflict of interest statement
Figures
Comment in
-
Community based health insurance in developing countries.BMJ. 2007 Jun 23;334(7607):1282-3. doi: 10.1136/bmj.39240.632963.80. BMJ. 2007. PMID: 17585121 Free PMC article.
References
-
- Gwatkin DR, Rustein S, Johnson K, Pande RP, Wagstaff A. Socio-economic differences in health, nutrition and population in India Washington, DC: World Bank, 2000
-
- Xu K, Evans DB, Kawabata K, Zeramdini R, Klavus J, Murray CJL. Household catastrophic health expenditure: a multicountry analysis. The Lancet 2003;362:111-7. - PubMed
-
- Schieber G, Baeza C, Kress D, Maier M. Financing health systems in the 21st century. In: Jamison DT, Breman JG, Measham AR, Alleyne G, Claeson M, Evans DB, et al, eds. Disease control priorities in developing countries 2nd ed. New York: Oxford University Press, 2006:1401.
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical