

Review
doi: 10.1102/1470-7330.2007.0010.
Laryngeal cancer: how does the radiologist help?
Affiliations
- PMID: 17535777
- PMCID: PMC1931513
- DOI: 10.1102/1470-7330.2007.0010
Item in Clipboard
Review
Laryngeal cancer: how does the radiologist help?
Cancer Imaging.
.
Abstract
The radiologist makes a valuable contribution to the staging of laryngeal cancer and this has a direct influence on treatment planning. This review focuses on the main anatomical concepts, patterns of tumour spread and how to detect this with optimal cross sectional imaging. Issues surrounding the relationship of tumour to the ventricular complex, submucosal laryngeal spaces, anteroposterior extension, laryngeal cartilage involvement and metastatic spread are discussed and illustrated. The impact of these imaging findings on the array of therapeutic options is described.
Figures

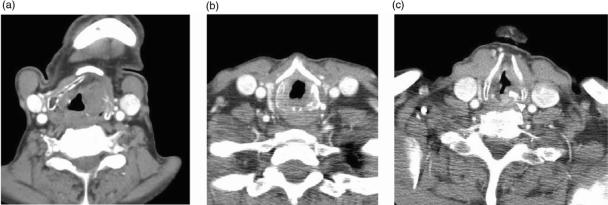
Axial CT scans through (a) false cords, (b) true cords, (c) subglottis to illustrate normal anatomy. (a) The tip of the arytenoids cartilages (white arrowhead) indicates the level of the false cords (open arrowhead) and also the superior aspect of the ventricular complex. (b) The anteriorly pointing vocal processes of the arytenoids (arrow) and the thyroarytenoid muscle (white arrowhead) are effacing the paraglottic fat within the wall of the larynx. This defines the level of the true cords and also the inferior aspect of the ventricular complex. The anterior and posterior (open arrowhead) commissures should only be represented by a thin mucosal layer. (c) There should be no soft tissue seen internal to the ring of the cricoid cartilage at subglottic level.
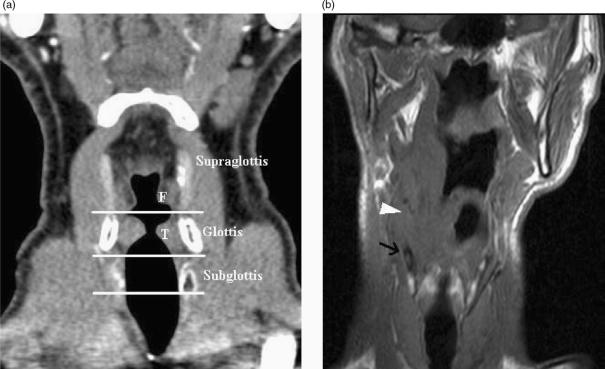
(a) Coronally reformatted CT demonstrates the supraglottis, glottis and subglottis as defined by the level of the ventricular complex (false cords (F), true cords (T) and intervening ventricle). (b) T1-w coronal image demonstrates a supraglottic tumour extending inferiorly to ventricular level (arrowhead). Low T1-w signal (arrow) in the thyroid cartilage is non specific for reactive change or tumour invasion.
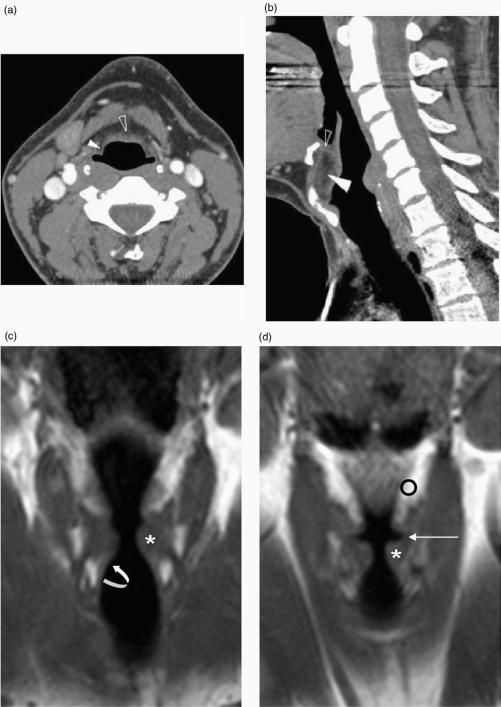
(a) Axial, (b) sagittal reformatted CT images with (c) and (d) T1-w coronal MR images illustrating the submucosal laryngeal spaces. (a) The pre-epiglottic space (open arrowhead) and paraglottic space (white arrowhead) are seen in continuity. (b) More superiorly the pre-epiglottic space (white arrowhead) is bound anteriorly by the thyrohyoid membrane (see also (a)) whereas the thyroid cartilage is present anteriorly at a more inferior level (see also Fig. 1a). The epiglottis is present posteriorly. Soft tissue seen within the superior aspect of the pre-epiglottic space (open arrowhead) corresponds to the hyoepiglottic ligament. (c) The medial relations of the paraglottic fat (o) are seen to be the vestibule, the ventricle (long arrow) and the conus elasticus more inferiorly (curved arrow). Laterally it is related to thyroid cartilage and cricothyroid membrane. The true vocal cord is indicated (*).
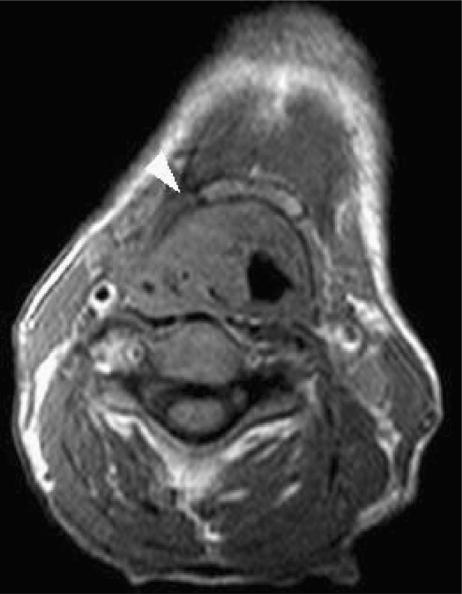
Axial T1-w image demonstrates bulky invasion of the right pre-epiglottic space by a supraglottic carcinoma which resulted in invasion of the hyoid bone.
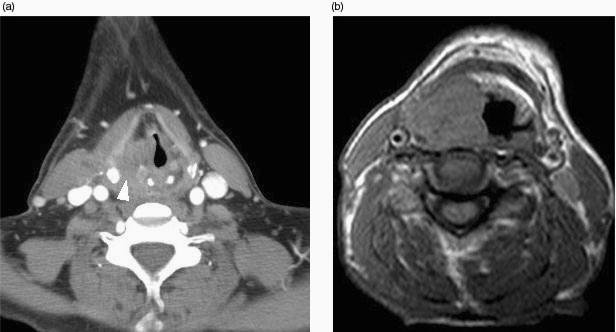
(a) Axial CT image demonstrates extension of paraglottic tumour to widen the thyroarytenoid gap and invade the piriform sinus submucosally. (b) Axial T1-w image illustrates how a bulky paraglottic tumour may extend laterally into the soft tissues of the neck through the thyrohyoid and cricohyoid membranes or through cartilage invasion. This tumour lies close to but does not encroach on the carotid sheath.

Axial CT scan shows thickening of the anterior commissure by glottic tumour (arrowhead).
Erosion of the thyroid cartilage (a) and cricoid cartilage (b) indicates cartilage involvement by tumour. Sclerosis (arrowhead) is less specific, however may be used as an indicator of cartilage involvement for the arytenoid (c) or cricoid cartilages.

Axial CT scan reveals a right sided necrotic lymph node secondary to a supraglottic carcinoma. The lymph node had not been palpated by the referring clinician.
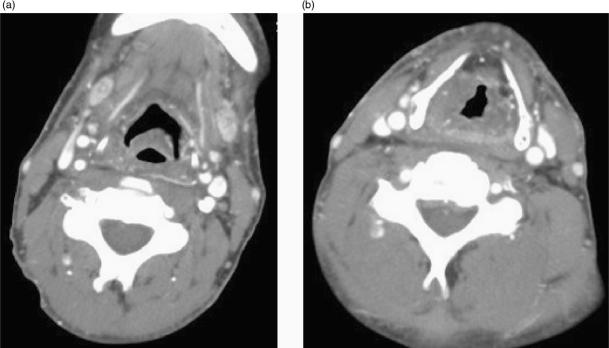
(a) Superiorly and b) inferiorly. Four months following radiotherapy for a supraglottic carcinoma, there are typical post radiotherapy appearances of oedematous thickening within supraglottic structures, thickening of fascial planes and streaky density within the fat spaces. The submandibular glands are atrophic and markedly enhancing.
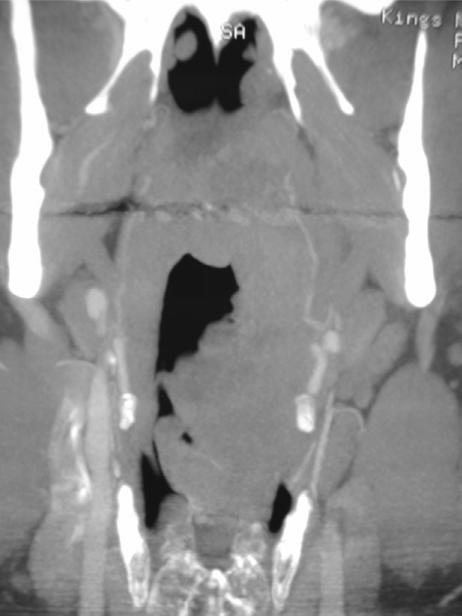
Coronally reformatted image from an advanced CT study demonstrates left sided supraglottic tumour. This corresponded to a venous malformation (cavernous haemangioma).
References
-
- Esteve J, Kricker A, Ferlay J, Parkin NM, editors. Lyon: World Health Organization; 1993. In: Facts and figures of cancer in the European Community. International Agency for Research on Cancer Commission of the European Communities.
-
- London: DoH; 2000. Department of Health Guidance Document HSC 2000/13 – Referral guidelines for suspected cancer.
-
- American Joint Committee on Cancer . Cancer staging handbook. 6th. New York: Springer; 2002. edn.
-
- Urba SG, Wolf GT, Bradford CA, et al. Neoadjuvant therapy for organ preservation in head and neck cancer. Laryngoscope. 2000;110:2074–80. - PubMed
-
- Magnano M, Bongioannini G, Cirillo S, et al. Virtual endoscopy of laryngeal carcinoma: is it useful? Otolaryngol Head Neck Surg. 2005;132:776–82. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical