

Electroacupuncture-induced analgesia in a rat model of ankle sprain pain is mediated by spinal alpha-adrenoceptors
- PMID: 17537577
- PMCID: PMC2268107
- DOI: 10.1016/j.pain.2007.04.034
Electroacupuncture-induced analgesia in a rat model of ankle sprain pain is mediated by spinal alpha-adrenoceptors
Abstract
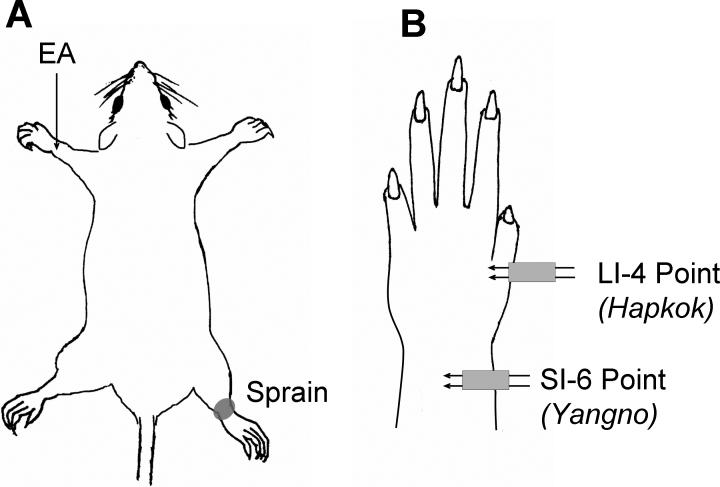
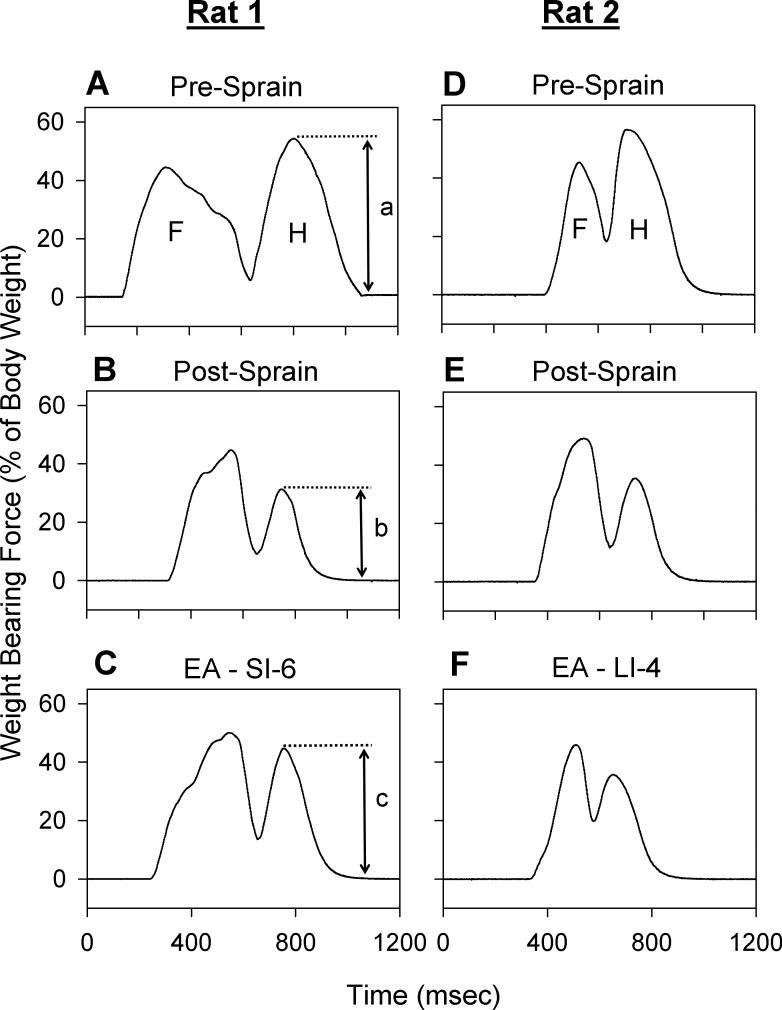
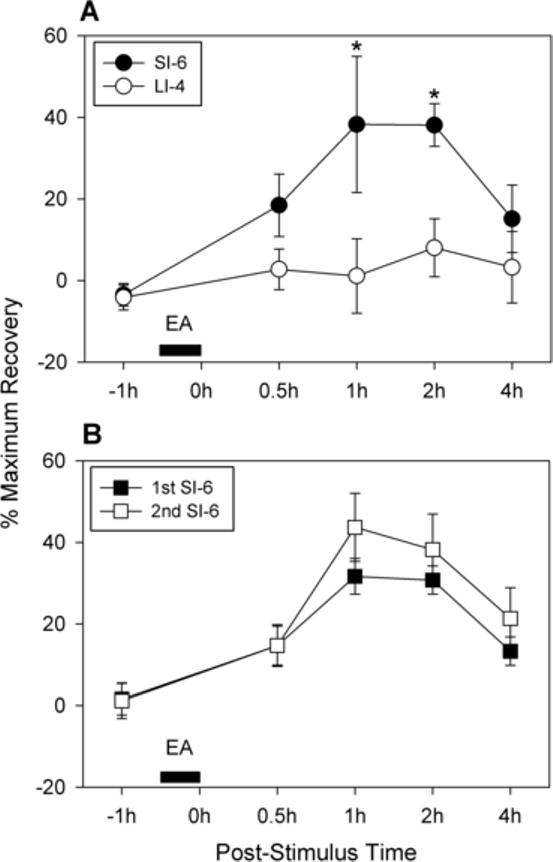
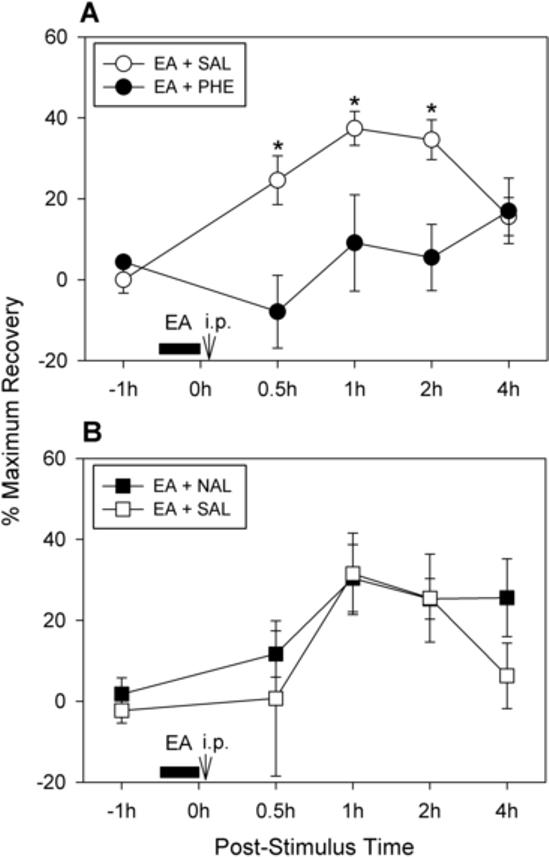
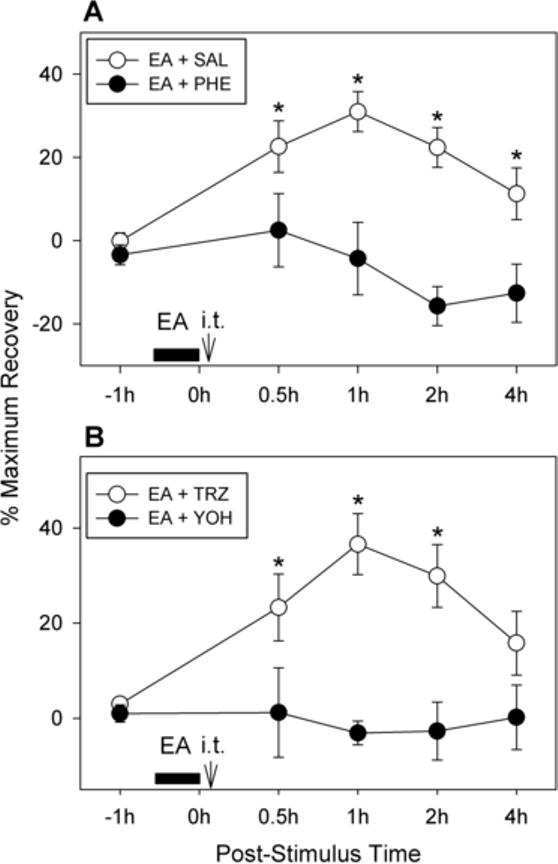
In a previous study, we showed that electroacupuncture (EA) applied to the SI-6 point on the contralateral forelimb produces long-lasting and powerful analgesia in pain caused by ankle sprain in a rat model. To investigate the underlying mechanism of EA analgesia, the present study tested the effects of various antagonists on known endogenous analgesic systems in this model. Ankle sprain was induced in anesthetized rats by overextending their right ankle with repeated forceful plantar flexion and inversion of the foot. When rats developed pain behaviors (a reduction in weight-bearing of the affected hind limb), EA was applied to the SI-6 point on the contralateral forelimb for 30 min under halothane anesthesia. EA significantly improved the weight-bearing capacity of the affected hind limb for 2h, suggesting an analgesic effect. The alpha-adrenoceptor antagonist phentolamine (2mg/kg, i.p. or 30 microg, i.t.) completely blocked the EA-induced analgesia, whereas naloxone (1mg/kg, i.p.) failed to block the effect. These results suggest that EA-induced analgesia is mediated by alpha-adrenoceptor mechanisms. Further experiments showed that intrathecal administration of yohimbine, an alpha(2)-adrenergic antagonist, reduced the EA-induced analgesia in a dose-dependent manner, whereas terazosin, an alpha(1)-adrenergic antagonist, did not produce any effect. These data suggest that the analgesic effect of EA in ankle sprain pain is, at least in part, mediated by spinal alpha(2)-adrenoceptor mechanisms.
Figures
References
-
- Akduman B, Crawford ED. Terazosin, doxazosin, and prazosin: current clinical experience. Urology. 2001;58(6 Suppl 1):49–54. - PubMed
-
- Bossut DF, Huang ZS, Sun SL, Mayer DJ. Electroacupuncture in rats: evidence for naloxone and naltrexone potentiation of analgesia. Brain Res. 1991;549:36–46. - PubMed
-
- Chapman CR, Benedetti C, Colpitts YH, Gerlach R. Naloxone fails to reverse pain thresholds elevated by acupuncture: acupuncture analgesia reconsidered. Pain. 1983;16:13–31. - PubMed
-
- Chapman CR, Colpitts YM, Benedetti C, Kitaeff R, Gehrig JD. Evoked potential assessment of acupunctural analgesia: attempted reversal with naloxone. Pain. 1980;9:183–197. - PubMed
-
- Cheng RSS, Pomeranz B. Monoaminergic mechanism of electroacupuncture analgesia. Brain Res. 1981;215:77–92. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
