

Vascular calcification in middle age and long-term risk of hip fracture: the Framingham Study
- PMID: 17542685
- PMCID: PMC2748402
- DOI: 10.1359/jbmr.070519
Vascular calcification in middle age and long-term risk of hip fracture: the Framingham Study
Abstract
Osteoporosis and atherosclerosis frequently occur in the same individuals and may share similar pathogenic mechanisms. This study examined the relation between severity of aortic calcification in middle-age years and subsequent risk of hip fracture in women and men in the population-based Framingham Study.
Introduction: We assessed vascular calcification in women and men in middle age and risk of hip fracture at advanced age.
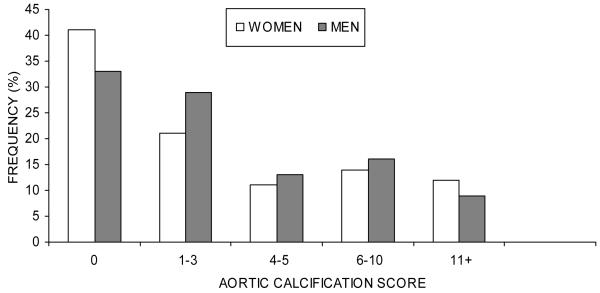
Materials and methods: Participants included 2499 Framingham cohort members (mean age, 61 yr; range, 47-80 yr). Semiquantitative methods were used to determine severity of abdominal aortic calcification on baseline radiographs. Information on potential confounding factors was obtained from study examinations conducted at, or before, baseline radiography. Hip fractures were ascertained by active surveillance and confirmed by medical records.
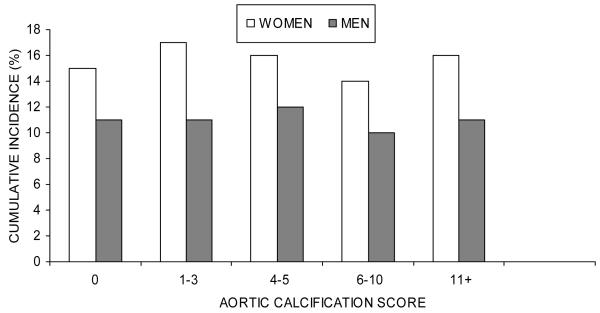
Results: Thirty-five-year cumulative incidence of hip fracture was 16% in women and 5% in men with prevalent aortic calcification at baseline (score 1+) and 14% in women and 4% in men without aortic calcification (score 0). Hazard ratios (HRs) and 95% CIs for hip fracture did not increase from the lowest to the highest category of aortic calcification. HRs were 1.0, 1.2 (95% CI, 0.9-1.8), 1.2 (95% CI, 0.7-1.9), 1.1 (95% CI, 0.7-1.7), and 1.4 (95% CI, 0.8-2.3) in women (p for trend = 0.44) and 1.0, 1.8 (95% CI, 0.8-3.8), 1.8 (95% CI, 0.7-4.6), 1.5 (95% CI, 0.6-3.9), and 1.2 (95% CI, 0.2-5.7) in men (p for trend = 0.29) for aortic calcification scores 0 (reference), 1-4, 4-5, 6-10, and 11+, respectively. However, aortic calcification score was strongly associated with increased risk of death (p for trend < 0.0001 in women and men). HRs (95% CIs) for mortality from the lowest to highest aortic calcification score were 1.0, 1.6 (1.4-1.9), 1.7 (1.4-2.1), 1.8 (1.5-2.2), and 2.1 (1.7-2.6) for women, and for men were 1.0, 1.4 (1.1-1.6), 1.4 (1.2-1.8), 1.6 (1.3-2.0), and 1.9 (1.5-2.5).
Conclusions: Vascular calcification in middle-aged adults does not increase long-term hip fracture risk.
Figures
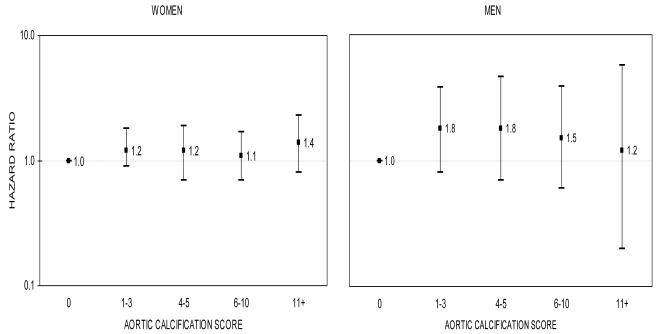
 bars denote 95 percent confidence intervals. * Models included baseline age, body mass index, systolic blood pressure, smoking, total cholesterol, diabetes, coronary heart disease, and estrogen use (in women).
bars denote 95 percent confidence intervals. * Models included baseline age, body mass index, systolic blood pressure, smoking, total cholesterol, diabetes, coronary heart disease, and estrogen use (in women).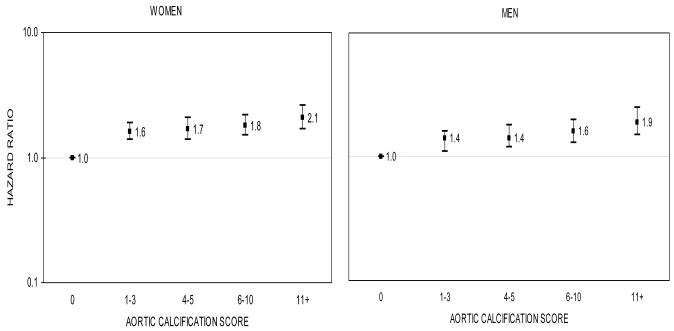
 bars denote 95 percent confidence intervals. * Models included baseline age, body mass index, systolic blood pressure, smoking, total cholesterol, diabetes, coronary heart disease, and estrogen use (in women).
bars denote 95 percent confidence intervals. * Models included baseline age, body mass index, systolic blood pressure, smoking, total cholesterol, diabetes, coronary heart disease, and estrogen use (in women).Similar articles
-
High hip fracture risk in men with severe aortic calcification: MrOS study.J Bone Miner Res. 2014 Apr;29(4):968-75. doi: 10.1002/jbmr.2085. J Bone Miner Res. 2014. PMID: 23983224 Free PMC article.
-
Association Between Abdominal Aortic Calcification, Bone Mineral Density, and Fracture in Older Women.J Bone Miner Res. 2019 Nov;34(11):2052-2060. doi: 10.1002/jbmr.3830. Epub 2019 Oct 9. J Bone Miner Res. 2019. PMID: 31310354 Clinical Trial.
-
Protective effect of total and supplemental vitamin C intake on the risk of hip fracture--a 17-year follow-up from the Framingham Osteoporosis Study.Osteoporos Int. 2009 Nov;20(11):1853-61. doi: 10.1007/s00198-009-0897-y. Epub 2009 Apr 4. Osteoporos Int. 2009. PMID: 19347239 Free PMC article.
-
Abdominal aortic calcification and risk of fracture among older women - The SOF study.Bone. 2015 Dec;81:16-23. doi: 10.1016/j.bone.2015.06.019. Epub 2015 Jun 24. Bone. 2015. PMID: 26115911 Free PMC article.
-
Association Between Body Mass Index and the Risk of Hip Fracture by Sex and Age: A Prospective Cohort Study.J Bone Miner Res. 2018 Sep;33(9):1603-1611. doi: 10.1002/jbmr.3464. Epub 2018 Jun 15. J Bone Miner Res. 2018. PMID: 29750839
Cited by
-
Is vascular calcification associated with bone mineral density and osteoporotic fractures in ambulatory, elderly women?Osteoporos Int. 2012 May;23(5):1533-9. doi: 10.1007/s00198-011-1762-3. Epub 2011 Sep 8. Osteoporos Int. 2012. PMID: 21901478
-
Osteoporosis in men: findings from the Osteoporotic Fractures in Men Study (MrOS).Ther Adv Musculoskelet Dis. 2016 Feb;8(1):15-27. doi: 10.1177/1759720X15621227. Ther Adv Musculoskelet Dis. 2016. PMID: 26834847 Free PMC article. Review.
-
The effect of risedronate (17.5 mg/week) treatment on quality of life in Japanese women with osteoporosis: a prospective observational study.J Bone Miner Metab. 2012 Nov;30(6):715-21. doi: 10.1007/s00774-012-0372-2. Epub 2012 Aug 7. J Bone Miner Metab. 2012. PMID: 22868656
-
The link between osteoporosis and cardiovascular disease.Clin Cases Miner Bone Metab. 2008 Jan;5(1):19-34. Clin Cases Miner Bone Metab. 2008. PMID: 22460842 Free PMC article.
-
Meta-analysis of hypertension and osteoporotic fracture risk in women and men.Osteoporos Int. 2017 Aug;28(8):2309-2318. doi: 10.1007/s00198-017-4050-z. Epub 2017 Apr 26. Osteoporos Int. 2017. PMID: 28447105
References
-
- Hofbauer LC, Schoppet M. Clinical implications of the osteoprotegerin/RANKL/RANK system for bone and vascular diseases. Jama. 2004;292(4):490–5. - PubMed
-
- Schoppet M, Preissner KT, Hofbauer LC. RANK ligand and osteoprotegerin: paracrine regulators of bone metabolism and vascular function. Arterioscler Thromb Vasc Biol. 2002;22(4):549–53. - PubMed
-
- Jie KG, Bots ML, Vermeer C, Witteman JC, Grobbee DE. Vitamin K status and bone mass in women with and without aortic atherosclerosis: a population-based study. Calcif Tissue Int. 1996;59(5):352–6. - PubMed
-
- Kammerer CM, Dualan AA, Samollow PB, Perisse AR, Bauer RL, MacCluer JW, O’Leary DH, Mitchell BD. Bone mineral density, carotid artery intimal medial thickness, and the vitamin D receptor BsmI polymorphism in Mexican American women. Calcif Tissue Int. 2004;75(4):292–8. - PubMed
-
- Parhami F. Possible role of oxidized lipids in osteoporosis: could hyperlipidemia be a risk factor? Prostaglandins Leukot Essent Fatty Acids. 2003;68(6):373–8. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
