

Rates and types of events reported to established incident reporting systems in two US hospitals
- PMID: 17545340
- PMCID: PMC2464990
- DOI: 10.1136/qshc.2006.019901
Rates and types of events reported to established incident reporting systems in two US hospitals
Abstract
Background: US hospitals have had voluntary incident reporting systems for many years, but the effectiveness of these systems is unknown. To facilitate substantial improvements in patient safety, the systems should capture incidents reflecting the spectrum of adverse events that are known to occur in hospitals.
Objective: To characterise the incidents from established voluntary hospital reporting systems.
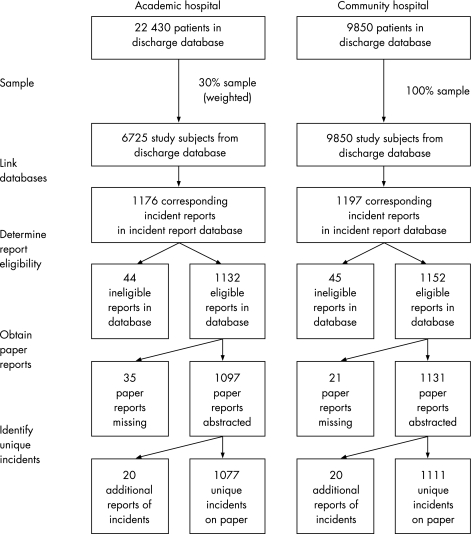
Design: Observational study examining about 1000 reports of hospitalised patients at each of two hospitals.
Patients and setting: 16 575 randomly selected patients from an academic and a community hospital in the US in 2001.
Main outcome measures: Rates of incidents reported per hospitalised patient and characteristics of reported incidents.
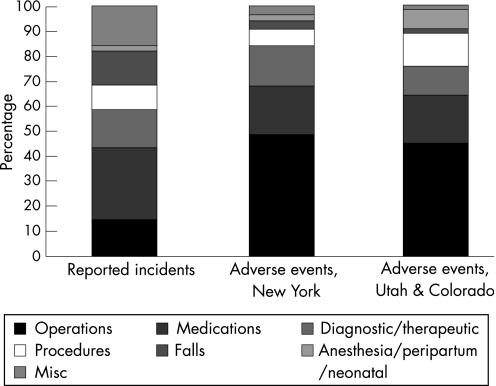
Results: 9% of patients had at least one reported incident; 17 incidents were reported per 1000 patient-days in hospital. Nurses filed 89% of reports, physicians 1.9% and other providers 8.9%. The most common types were medication incidents (29%), falls (14%), operative incidents (15%) and miscellaneous incidents (16%); 59% seemed preventable and preventability was not clear for 32%. Among the potentially preventable incidents, 43% involved nurses, 16% physicians and 19% other types of providers. Qualitative examination of reports indicated that very few involved prescribing errors or high-risk procedures.
Conclusions: Hospital reporting systems receive many reports, but capture a spectrum of incidents that differs from the adverse events known to occur in hospitals, thereby substantially underdetecting physician incidents, particularly those involving operations, high-risk procedures and prescribing errors. Increasing the reporting of physician incidents will be essential to enhance the effectiveness of hospital reporting systems; therefore, barriers to reporting such incidents must be minimised.
Conflict of interest statement
Competing interests: None.
References
-
- Agency for Healthcare Research and Quality Detail of performance analysis table, quality/safety of patient safety portfolio. Budget estimates for Appropriations Committees, fiscal year 2006. Available at: http://www.ahrq.gov/about/cj2006/cj06exbua.htm (accessed 31 Mar 2007)
-
- S 544. The Patient Safety and Quality Improvement Act of2005
-
- United Kingdom National Patient Safety Agency Seven steps to patient safety—your guide to safer patient care. Available at: http://www.npsa.nhs.uk/health/resources/7steps (accessed 31 Mar 2007)
-
- Runciman W B. Iatrogenic injury in Australia. A report by the Australian Patient Safety Foundation for the National Health Priorities and Quality Branch. Canberra, 2000. Available at: http://www.apsf.net.au/dbfiles/Iatrogenic_Injury.pdf (accessed 31 Mar 2007)
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources