

Why poor quality of ethnicity data should not preclude its use for identifying disparities in health and healthcare
- PMID: 17545342
- PMCID: PMC2465001
- DOI: 10.1136/qshc.2006.019059
Why poor quality of ethnicity data should not preclude its use for identifying disparities in health and healthcare
Abstract
Background: Data of quality are needed to identify ethnic disparities in health and healthcare and to meet the challenges in governance of race relations. Yet concerns over completeness, accuracy and timeliness have been long-standing and inhibitive with respect to the analytical use of the data.
Aims: To identify incompleteness of ethnicity data across routine health and healthcare datasets and to investigate the utility of analytical strategies for using data that is of suboptimal quality.
Methods: An analysis by government office regions of ethnicity data incompleteness in routine datasets and a comprehensive review and evaluation of the literature on appropriate analytical strategies to address the use of such data.
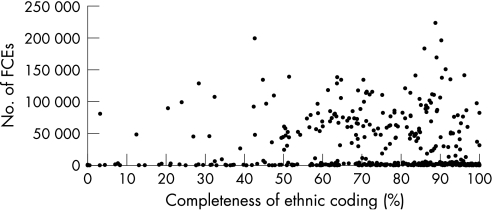
Results: There is only limited availability of ethnically coded routine datasets on health and healthcare, with substantial variability in valid ethnic coding: although a few have high levels of completeness, the majority are poor (notably hospital episode statistics, drug treatment data and non-medical workforce). In addition, there is also a more than twofold regional difference in quality. Organisational factors seem to be the main contributor to the differentials, and these are amenable-yet, in practice, difficult-to change. This article discusses the strengths and limitations of a variety of analytical strategies for using data of suboptimal quality and explores how they may answer important unresolved questions in relation to ethnic inequalities.
Conclusions: Only by using the data, even when of suboptimal quality, and remaining close to it can healthcare organisations drive up quality.
Conflict of interest statement
Competing interests: None.
References
-
- Aspinall P J. Secondary analysis of administrative, routine and research data sources: lessons from the UK. In: Nazroo JY, ed. Health and social research in multiethnic societies. London: Routledge, 2006165–195.
-
- Fitzpatrick J, Jacobson B, Aspinall P J.Indications of public health in the English regions. Vol 4. Ethnicity and health. London: Association of Public Health Observatories, 2005
-
- HES Data Quality Indicator Report for data year 2003/2004. http://www. hesonline.nhs.uk/Ease/servlet/ContentServer?siteID = 1937&categoryID = 452
-
- Platt L, Akinwale B, Simpson L. Stability and change in ethnic group in England and Wales. Popul Trends 200512135–45. - PubMed
-
- Goldacre M J. The Oxford Record Linkage Study: current position and future prospects. In: Howe GR, Spasoff RA, eds. Proceedings of the Workshop on Computerised Record Linkage in Health Research. Toronto: University of Toronto Press, 1986106–129.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources