

Concordance between routine interictal magnetoencephalography and simultaneous scalp electroencephalography in a sample of patients with epilepsy
- PMID: 17545825
- PMCID: PMC4096347
- DOI: 10.1097/WNP.0b013e3180556095
Concordance between routine interictal magnetoencephalography and simultaneous scalp electroencephalography in a sample of patients with epilepsy
Abstract
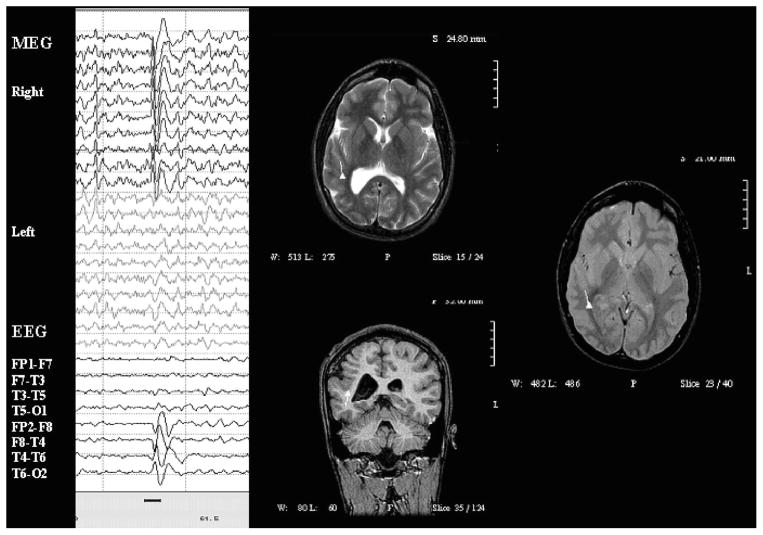
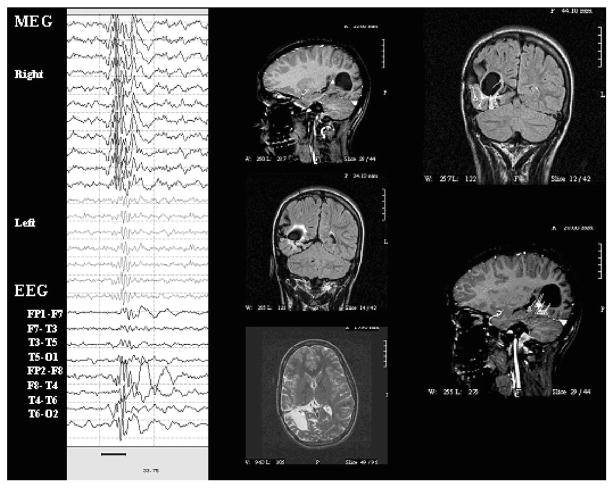
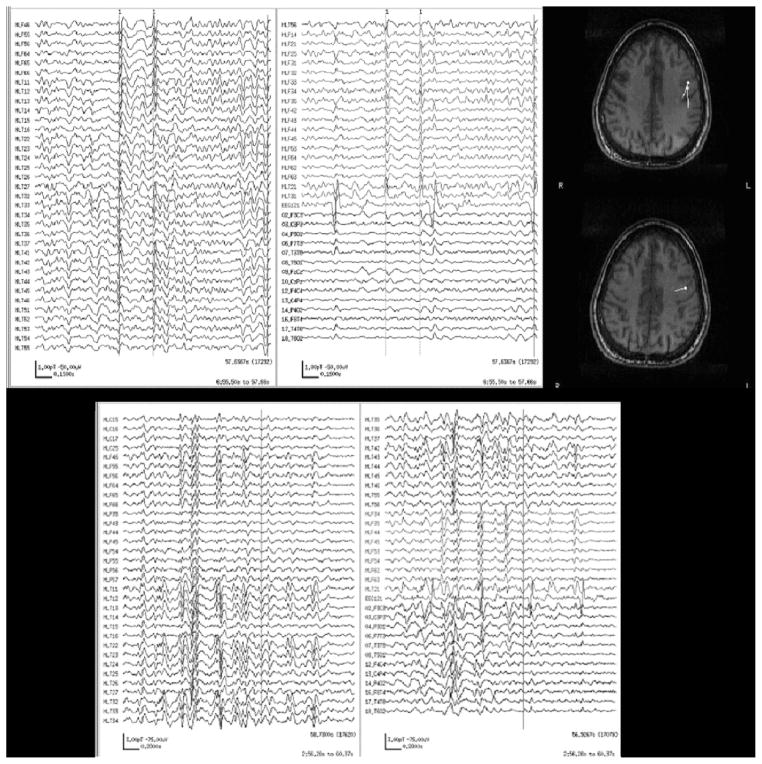
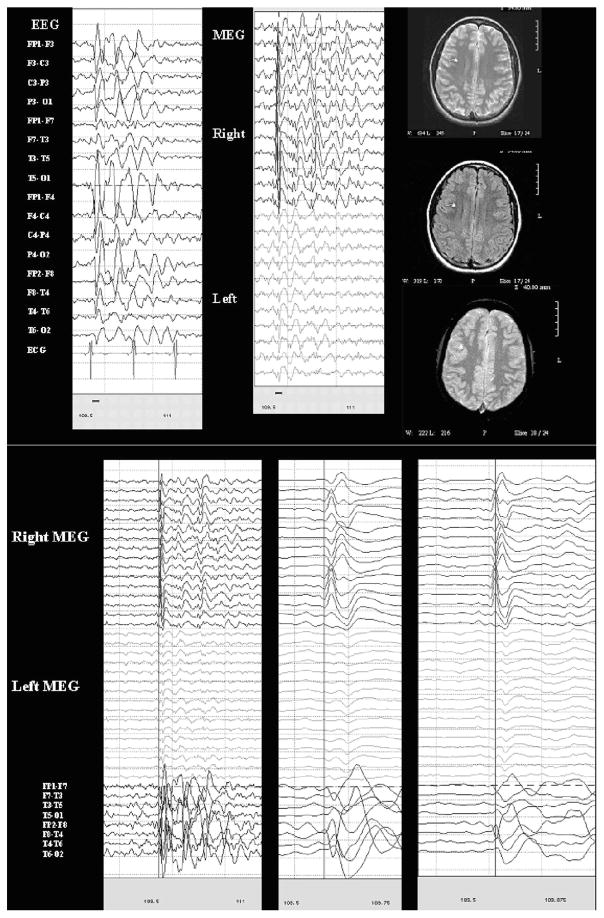
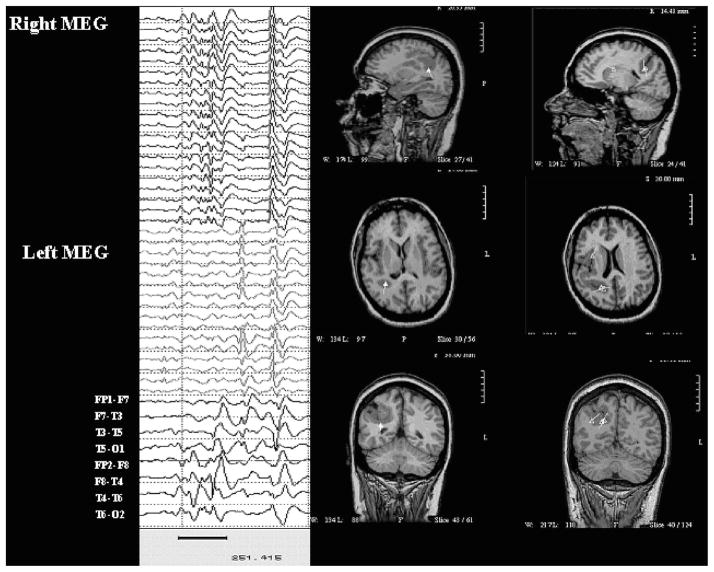
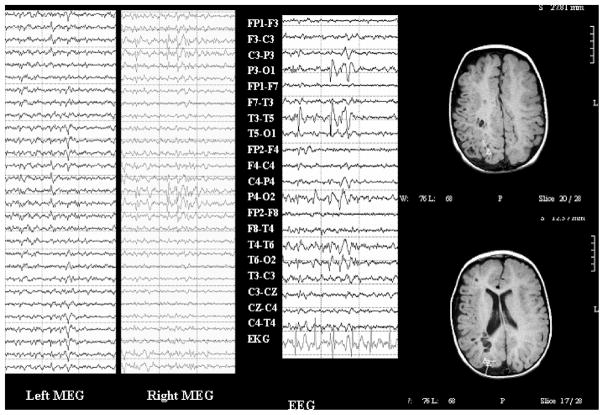
Both electroencephalography (EEG) and magnetoencephalography (MEG) localize epileptiform activity but may yield different results. This discordance may arise from different detection capabilities or from different data collection and interpretation techniques. Comparisons of MEG and EEG have focused on detection of individual spikes. However, side-by-side comparisons of results as used in the clinical setting is lacking. In this report, we present our empirical comparison. We reviewed 58 simultaneous MEG-EEG recordings (35 paired-sensors, 23 whole-head) from a diverse epilepsy population, comparing previous clinical MEG interpretations with new blinded EEG interpretations, noting lobar concordance of readers' judgments of regional abnormalities. A second-pass unblinded analysis, using all available clinical data, assessed the relative contribution and plausibility of the results of each technique. Concordance was high (85%) overall. Discordance was sometimes caused by constraints imposed by MEG dipole fitting techniques. Even when results of the techniques did not match, MEG often disambiguated the clinical scenario, especially when combined with imaging information. Thoughtful analysis of combined MEG-EEG datasets, beyond algorithm-based interictal spike detection, can help guide clinical decision-making even when concordance between techniques is imperfect. In some cases, EEG and MEG are synergistic and provide complementary information.
Figures
References
-
- Commission on Classification and Terminology of the International League Against Epilepsy. Proposal for revised classification of epilepsies and epileptic syndromes. Epilepsia. 1989;30:389–399. - PubMed
-
- Barkley GL, Baumgartner C. MEG and EEG in epilepsy. J Clin Neurophysiol. 2003;20:163–178. - PubMed
-
- Bast T, Ramantani G, Boppel T, et al. Source analysis of interictal spikes in polymicrogyria: loss of relevant cortical fissures requires simultaneous EEG to avoid MEG misinterpretation. Neuroimage. 2005;25:1232–1241. - PubMed
-
- Baumgartner C. Controversies in clinical neurophysiology: MEG is superior to EEG in the localization of interictal epileptiform activity: con. Clin Neurophysiol. 2004;115:1010–1020. - PubMed
-
- Fuchs M, Wagner M, Wischmann HA, et al. Improving source reconstructions by combining bioelectric and biomagnetic data. Electroencephalogr Clin Neurophysiol. 1998;107:93–111. - PubMed
