

Duplex ultrasonography, magnetic resonance angiography, and computed tomography angiography for diagnosis and assessment of symptomatic, lower limb peripheral arterial disease: systematic review
- PMID: 17548364
- PMCID: PMC1892528
- DOI: 10.1136/bmj.39217.473275.55
Duplex ultrasonography, magnetic resonance angiography, and computed tomography angiography for diagnosis and assessment of symptomatic, lower limb peripheral arterial disease: systematic review
Abstract
Objectives: To determine the diagnostic accuracy of duplex ultrasonography, magnetic resonance angiography, and computed tomography angiography, alone or in combination, for the assessment of lower limb peripheral arterial disease; to evaluate the impact of these assessment methods on management of patients and outcomes; and to evaluate the evidence regarding attitudes of patients to these technologies and summarise available data on adverse events.
Design: Systematic review.
Methods: Searches of 11 electronic databases (to April 2005), six journals, and reference lists of included papers for relevant studies. Two reviewers independently selected studies, extracted data, and assessed quality. Diagnostic accuracy studies were assessed for quality with the QUADAS checklist.
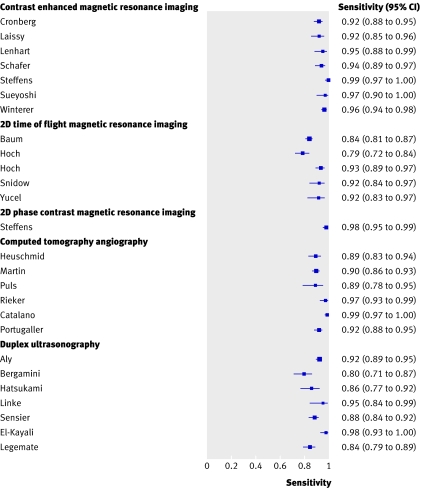
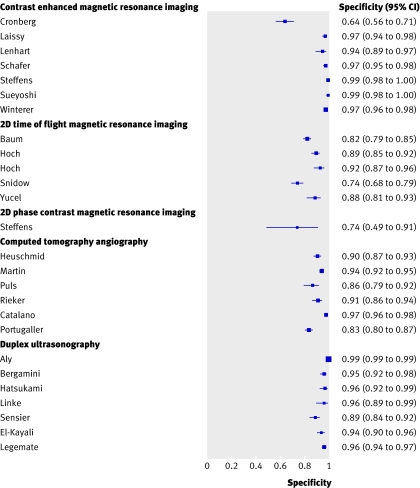
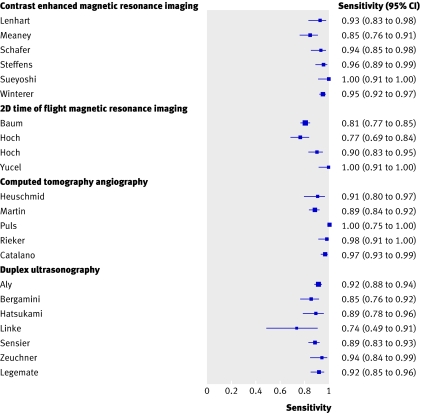
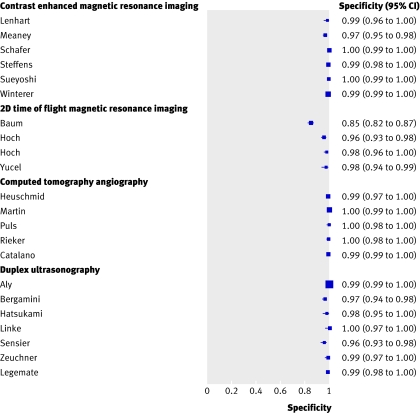
Results: 107 studies met the inclusion criteria; 58 studies provided data on diagnostic accuracy, one on outcomes in patients, four on attitudes of patients, and 44 on adverse events. Quality assessment highlighted limitations in the methods and quality of reporting. Most of the included studies reported results by arterial segment, rather than by limb or by patient, which does not account for the clustering of segments within patients, so specificities may be overstated. For the detection of stenosis of 50% or more in a lower limb vessel, contrast enhanced magnetic resonance angiography had the highest diagnostic accuracy with a median sensitivity of 95% (range 92-99.5%) and median specificity of 97% (64-99%). The results were 91% (89-99%) and 91% (83-97%) for computed tomography angiography and 88% (80-98%) and 96% (89-99%) for duplex ultrasonography. A controlled trial reported no significant differences in outcomes in patients after treatment plans based on duplex ultrasonography alone or conventional contrast angiography alone, though in 22% of patients supplementary contrast angiography was needed to form a treatment plan. The limited evidence available suggested that patients preferred magnetic resonance angiography (with or without contrast) to contrast angiography, with half expressing no preference between magnetic resonance angiography or duplex ultrasonography (among patients with no contraindications for magnetic resonance angiography, such as claustrophobia). Where data on adverse events were available, magnetic resonance angiography was associated with the highest proportion of adverse events, but these were mild. The most severe adverse events, although rare, were mainly associated with contrast angiography.
Conclusions: Contrast enhanced magnetic resonance angiography seems to be more specific than computed tomography angiography (that is, better at ruling out stenosis over 50%) and more sensitive than duplex ultrasonography (that is, better at ruling in stenosis over 50%) and was generally preferred by patients over contrast angiography. Computed tomography angiography was also preferred by patients over contrast angiography; no data on patients' preference between duplex ultrasonography and contrast angiography were available. Where available, contrast enhanced magnetic resonance angiography might be a viable alternative to contrast angiography.
Conflict of interest statement
Figures
Comment in
-
Diagnosis of peripheral arterial disease of the lower limb.BMJ. 2007 Jun 16;334(7606):1229-30. doi: 10.1136/bmj.39244.344664.80. BMJ. 2007. PMID: 17569893 Free PMC article.
-
Gadolinium contrast may be risky in kidney disease.BMJ. 2007 Jun 30;334(7608):1335-6. doi: 10.1136/bmj.39254.924641.1F. BMJ. 2007. PMID: 17599982 Free PMC article. No abstract available.
-
Review: contrast-enhanced MRA is more sensitive and specific than CT angiography or ultrasonography for detection of lower-limb PAD.ACP J Club. 2007 Nov-Dec;147(3):77. ACP J Club. 2007. PMID: 17975879 No abstract available.
References
-
- Drug treatment of peripheral arterial disease. Bandolier 1996:29-34. www.jr2.ox.ac.uk/bandolier/band29/b29-4.html
-
- TransAtlantic Inter-Society Consensus (TASC). 2005. Management of peripheral arterial disease (PAD).www.tasc-pad.org/html/homepage.htm
-
- Collins R, Cranny G, Burch J, Aguiar-Ibáñez R, Craig D, Wright K, et al. A systematic review of duplex ultrasound, magnetic resonance angiography and computed tomography angiography for the diagnosis and assessment of symptomatic, lower limb peripheral arterial disease. Health Technol Assess 2007;11:1-202. - PubMed
-
- Whiting P, Rutjes A, Reitsma J, Bossuyt P, Kleijnen J. The development of QUADAS: a tool for the quality assessment of studies of diagnostic accuracy included in systematic reviews. BMC Med Res Methodol 2003;3. www.biomedcentral.com/1471-2288/3/25 - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous