

Competing demands or clinical inertia: the case of elevated glycosylated hemoglobin
- PMID: 17548846
- PMCID: PMC1886492
- DOI: 10.1370/afm.679
Competing demands or clinical inertia: the case of elevated glycosylated hemoglobin
Abstract
Purpose: This study aimed to examine the contribution of competing demands to changes in hypoglycemic medications and to return appointment intervals for patients with type 2 diabetes and an elevated glycosylated hemoglobin (A1c) level.
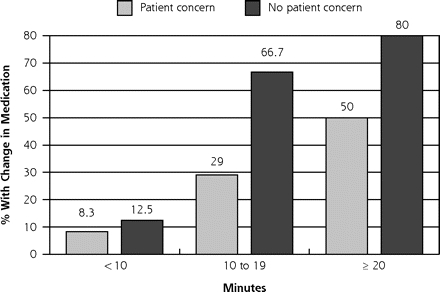
Methods: We observed 211 primary care encounters by adult patients with type 2 diabetes in 20 primary care clinics and documented changes in hypoglycemic medications. Competing demands were assessed from length of encounter, number of concerns patients raised, and number of topics brought up by the clinician. Days to the next scheduled appointment were obtained at patient checkout. Recent A1c values and dates were determined from the chart.
Results: Among patients with an A(1c) level greater than 7%, each additional patient concern was associated with a 49% (95% confidence interval, 35%-60%) reduction in the likelihood of a change in medication, independent of length of the encounter and most recent level of A1c. Among patients with an A(1c) level greater than 7% and no change in medication, for every additional minute of encounter length, the time to the next scheduled appointment decreased by 2.8 days (P = .001). Similarly, for each additional 1% increase in A1c level, the time to the next scheduled appointment decreased by 8.6 days (P=.001).
Conclusions: The concept of clinical inertia is limited and does not fully characterize the complexity of primary care encounters. Competing demands is a principle for constructing models of primary care encounters that are more congruent with reality and should be considered in the design of interventions to improve chronic disease outcomes in primary care settings.
Figures
References
-
- Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). UK Prospective Diabetes Study (UKPDS) Group. Lancet. 1998;352(9131):837–853. - PubMed
-
- Selvin E, Marinopoulos S, Berkenblit G, et al. Meta-analysis: glycosylated hemoglobin and cardiovascular disease in diabetes mellitus. Ann Intern Med. 2004;141(6):421–431. - PubMed
-
- American Diabetes Association. Clinical Practice Recommendations 2005. Diabetes Care. 2005;28(Suppl 1):S1–S79. - PubMed
-
- Harris MI, Eastman RC, Cowie CC, Flegal KM, Eberhardt MS. Racial and ethnic differences in glycemic control of adults with type 2 diabetes. Diabetes Care. 1999;22(3):403–408. - PubMed
-
- Imperatore G, Cadwell BL, Geiss L, et al. Thirty-year trends in cardiovascular risk factor levels among US adults with diabetes: National Health and Nutrition Examination Surveys, 1971–2000. Am J Epidemiol. 2004;160(6):531–539. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical