

Evidence-based protocol for structural rehabilitation of the spine and posture: review of clinical biomechanics of posture (CBP) publications
- PMID: 17549209
- PMCID: PMC1840024
Evidence-based protocol for structural rehabilitation of the spine and posture: review of clinical biomechanics of posture (CBP) publications
Abstract
Background: Although practice protocols exist for SMT and functional rehabilitation, no practice protocols exist for structural rehabilitation. Traditional chiropractic practice guidelines have been limited to acute and chronic pain treatment, with limited inclusion of functional and exclusion of structural rehabilitation procedures.
Objective: (1) To derive an evidence-based practice protocol for structural rehabilitation from publications on Clinical Biomechanics of Posture (CBP((R))) methods, and (2) to compare the evidence for Diversified, SMT, and CBP((R)).
Methods: Clinical control trials utilizing CBP(R) methods and spinal manipulative therapy (SMT) were obtained from searches in Mantis, CINAHL, and Index Medicus. Using data from SMT review articles, evidence for Diversified Technique (as taught in chiropractic colleges), SMT, and CBP((R)) were rated and compared.
Results: From the evidence from Clinical Control Trials on SMT and CBP((R)), there is very little evidence support for Diversified (our rating = 18), as taught in chiropractic colleges, for the treatment of pain subjects, while CBP((R)) (our rating = 46) and SMT for neck pain (rating = 58) and low back pain (our rating = 202) have evidence-based support.
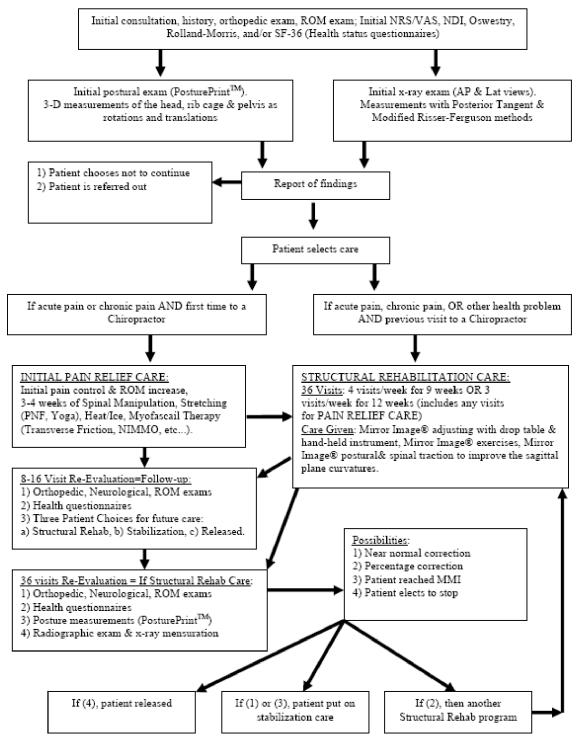
Conclusions: While CBP((R)) Technique has approximately as much evidence-based support as SMT for neck pain, CBP((R)) has more evidence to support its methods than the Diversified technique taught in chiropractic colleges, but not as much as SMT for low back pain. The evolution of chiropractic specialization has occurred, and doctors providing structural-based chiropractic care require protocol guidelines for patient quality assurance and standardization. A structural rehabilitation protocol was developed based on evidence from CBP((R)) publications.
ANTÉCÉDENTS: Quoi qu’il y ait des protocoles d’exercice établis pour la manipulation vertébrale et la réadaptation fonctionnelle, il n’existe aucun protocole pour la réadaptation structurale. Les directives d’exercices chiropratiques traditionnels se limitent à des traitements pour la douleur aigue et chronique avec une inclusion limitée des procédures de réadaptation fonctionnelle et une exclusion des procédures de réadaptation stucturale.
OBJECTIF: (1) Faire dévier des publications sur les procédures biomécaniques cliniques de la posture (BCP) un protocole d’exercice, avec preuve à l’appui, pour la réadaptation structurale, et (2) Comparer la preuve pour la techniques diversifiée, la manipulation vertébrale et la procédure biomécanique de la posture (BCP).
PROCÉDURES: Des essais de contrôle clinique avec l’utilisation des procédures biomécaniques cliniques et la manipulation vertébrale ont été obtenus, suite à des recherches dans Mantis, CINAHL et Index Medicus. En utilisant, les données des rapports de synthèse sur la manipulation vertébrale pour la technique diversifiée (tel qu’enseigné dans les collèges de chiropractie), la manipulation vertébrale et les procédures BCP ont été évaluées et comparées.
RÉSULTATS: Fondés sur la preuve des essais de contrôle clinique sur la manipulation vertébrale et les procédures BCP, il existe peu de preuve pour soutenir la technique diversifiée (notre taux = 18), tel qu’enseigné dans les collèges de chiropractie, pour le traitement de la douleur des sujets, contrairement aux procédures BCP (notre taux = 46) et la manipulation vertébrale pour la cervicalgie (taux = 58) et le lumbago (notre taux = 202) qui sont soutenues par la preuve.
CONCLUSION: Tandis que la procédure BCP possède approximativement, autant de preuve à l’appui que la manipulation vertébrale pour la cervicalgie, la méthode BCP possède davantage de preuves à l’appui, pour soutenir ses procédures que la méthode diversifiée, enseignée dans les collèges de chiropractie, mais pas autant que la manipulation vertébrale pour le lumbago. L’évolution de la spécialisation de la chiropractie est devenue une réalité et les médecins qui fournissent des soins de chiropractie, à base structurale, nécessitent des directives de protocole pour offrir aux patients une assurance de la qualité des soins et une normalisation. Un protocole de réadaptation structurale a été élaboré, fondé sur la preuve des publications, reliées aux procédures BCP.
Figures
Comment in
-
Flawed trials, flawed analysis: why CBP should avoid rating itself.J Can Chiropr Assoc. 2006 Jun;50(2):97-102. J Can Chiropr Assoc. 2006. PMID: 17549172 Free PMC article. No abstract available.
References
-
- Bolton JE. The evidence in evidence-based practice: what counts and what doesn’t count? J Manipulative Physiol Ther. 2001;24:362–366. - PubMed
-
- Sackett DL, Richardson WS, Rosenberg W, Haynes RB. Evidence-based medicine: How to practice and teach EBM. New York: Churchill-Livingstone, 1997.
-
- Lipman G. Evidence-based pain management and palliative care. J Pain Palliat Care Pharmacother. 2002;16:1–3. - PubMed
-
- Fishbain DA, Cutler RB, Rosomoff HL, Rosomoff RS. Can patients taking opioids drive safely? A structured evidence-based review. J Pain Palliat Care Pharmacother. 2002;16:9–28. - PubMed
-
- Caramanica L, Cousino JA, Peterson S. Four elements of a successful quality program. alignment, collaboration, evidence-based practice, and excellence. Nurs Adm Q. 2003;27:336–343. - PubMed
LinkOut - more resources
Full Text Sources