

Quality of clinical primary care and targeted incentive payments: an observational study
- PMID: 17550669
- PMCID: PMC2078183
Quality of clinical primary care and targeted incentive payments: an observational study
Abstract
Background: Payments for recorded evidence of quality of clinical care in UK general practices were introduced in 2004.
Aim: To examine the relationship between changes in recorded quality of care for four common chronic conditions from, 2003 to 2005, and the payment of incentives.
Design of study: Retrospective observational study comparing incentivised and non-incentivised indicators of quality of care.
Setting: Eighteen general practices in England.
Method: Medical records were examined for 1156 patients. The percentage of eligible quality indicators achieved for each patient was assessed in 2003 and 2005. Twenty-one quality indicators referred to asthma and hypertension: six subject to and 15 not subject to incentive payments. Another 15 indicators referred to depression and osteoarthritis which were not subject to incentive payments.
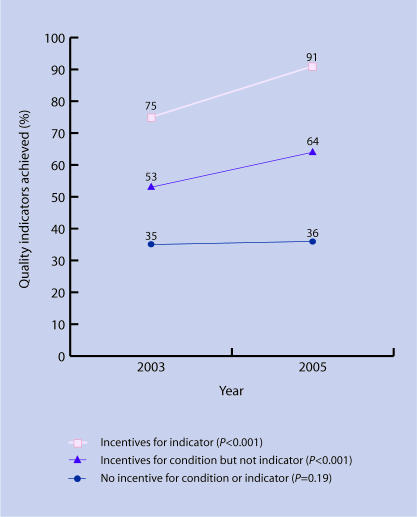
Results: A significant increase occurred for the six indicators linked to incentive payments: from 75% achieved in 2003 to 91% in 2005 (change = 16%, 95% confidence interval [CI] = 10 to 22%, P <0.01). A significant increase also occurred for 15 other indicators linked to 'incentivised conditions'; 53 to 64% (change = 11%, 95% CI = 6 to 15%, P <0.01). The 'non-incentivised conditions' started at a lower achievement level, and did not increase significantly: 35 to 36% (change = 2%, 95% CI = -1 to 4%, P = 0.19).
Conclusion: The introduction of financial incentives was associated with substantial apparent quality improvement for incentivised conditions. For non-incentivised conditions, quality did not appear to improve. Patients with non-incentivised conditions may be at risk of poorer quality care.
Figures
References
-
- General Practitioners Committee BMA, The NHS Confederation. Investing in general practice. The new General Medical Services contract. London: The NHS Confederation; 2003.
-
- Doran T, Fullwood C, Gravelle H, et al. Pay-for-performance programs in family practices in the United Kingdom. New Engl J Med. 2006;355:375–384. - PubMed
-
- Fleetcroft R, Cookson R. Do the incentive payments in the new NHS contract for primary care reflect likely population health gains? J Health Serv Res Policy. 2006;11:27–31. - PubMed
-
- Roland M. Linking physicians' pay to the quality of care — a major experiment in the United Kingdom. New Engl J Med. 2004;351:1448–1454. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources