

Resistant tennis elbow: shock-wave therapy versus percutaneous tenotomy
- PMID: 17551726
- PMCID: PMC2551723
- DOI: 10.1007/s00264-007-0379-9
Resistant tennis elbow: shock-wave therapy versus percutaneous tenotomy
Abstract
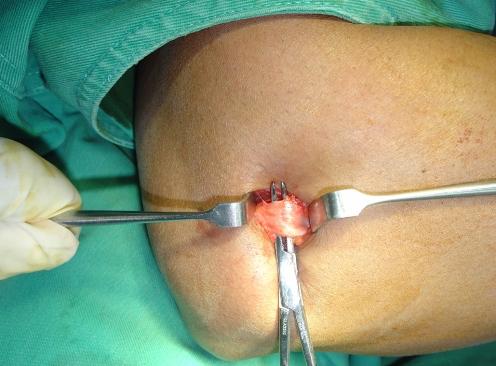
Fifty-six patients who suffered from chronic persistent tennis elbow of more than six months duration were randomly assigned to two active treatment groups. Group 1 (n = 29) received high-energy extracorporeal shock wave treatment (ESWT; 1,500 shocks) at 18 kV (0.22 mJ/mm(2)) without local anaesthesia; group 2 (n = 27) underwent percutaneous tenotomy of the common extensor origin. Both groups achieved improvement from the base line at three weeks, six weeks, 12 weeks and 12 months post-intervention. The success rate (Roles and Maudsley score: excellent and good) at three months in the ESWT group was 65.5% and in the tenotomy group was 74.1%. ESWT appeared to be a useful noninvasive treatment method that reduced the necessity for surgical procedures.
Cinquante-six patients qui souffraient de douleurs chroniques de type tennis elbow depuis plus de six mois ont été randomisés dans une étude avec deux groupes de traitements. Le groupe 1 (n = 29) a été traité par un traitement physique comprenant 1.500 chocs à 18 kV (0.22 mJ/mm2) après anesthésie locale, le groupe 2 (n = 27) a été traité par ténotomie percutanée de l’insertion de l’extenseur commun. Les deux groupes ont été évalués à 3 semaines, 6 semaines, 12 semaines et 12 mois après l’intervention au traitement. Le taux de bons résultats (selon le score de Roles et Maudsley) pour le groupe ayant bénéficié de traitements physiques a été de 65.5%, alors que le groupe traité par ténotomie présentait 74.1% de bons résultats. Le traitement physique apparaît utile. Il s’agit d’un traitement non invasif qui peut réduire la nécessité d’un traitement chirurgical.
Figures
Similar articles
-
Extracorporeal shock wave therapy in the treatment of lateral epicondylitis : a randomized multicenter trial.J Bone Joint Surg Am. 2002 Nov;84(11):1982-91. doi: 10.2106/00004623-200211000-00012. J Bone Joint Surg Am. 2002. PMID: 12429759 Clinical Trial.
-
A prospective, randomised study to compare extracorporeal shock-wave therapy and injection of steroid for the treatment of tennis elbow.J Bone Joint Surg Br. 2002 Jul;84(5):678-9. doi: 10.1302/0301-620x.84b5.12741. J Bone Joint Surg Br. 2002. PMID: 12188483 Clinical Trial.
-
[Principle and application of orthopedic ESWT apparatus].Zhongguo Yi Liao Qi Xie Za Zhi. 2010 Jul;34(4):297-9. Zhongguo Yi Liao Qi Xie Za Zhi. 2010. PMID: 21033121 Clinical Trial. Chinese.
-
Effectiveness of extracorporeal shock wave therapy for tennis elbow (lateral epicondylitis).Br J Sports Med. 2005 Mar;39(3):132-6. doi: 10.1136/bjsm.2004.015545. Br J Sports Med. 2005. PMID: 15728688 Free PMC article. Review.
-
Extracorporeal shock wave therapy for tendinopathies.Expert Rev Med Devices. 2006 Jul;3(4):463-70. doi: 10.1586/17434440.3.4.463. Expert Rev Med Devices. 2006. PMID: 16866643 Review.
Cited by
-
Extracorporeal shockwave therapy in musculoskeletal disorders.J Orthop Surg Res. 2012 Mar 20;7:11. doi: 10.1186/1749-799X-7-11. J Orthop Surg Res. 2012. PMID: 22433113 Free PMC article. Review.
-
Mechanical Stimulation (Pulsed Electromagnetic Fields "PEMF" and Extracorporeal Shock Wave Therapy "ESWT") and Tendon Regeneration: A Possible Alternative.Front Aging Neurosci. 2015 Nov 9;7:211. doi: 10.3389/fnagi.2015.00211. eCollection 2015. Front Aging Neurosci. 2015. PMID: 26617513 Free PMC article. Review.
-
Short- to mid-term follow-up effectiveness of US-guided focal extracorporeal shock wave therapy in the treatment of elbow lateral epicondylitis.Musculoskelet Surg. 2015 Sep;99 Suppl 1:S91-7. doi: 10.1007/s12306-015-0361-4. Epub 2015 May 10. Musculoskelet Surg. 2015. PMID: 25957547
-
[Treatment of lateral and medial epicondylopathy : Are platelet-rich plasma, shock wave therapy, etc. effective for both?].Orthopadie (Heidelb). 2023 May;52(5):371-378. doi: 10.1007/s00132-023-04372-8. Epub 2023 Apr 13. Orthopadie (Heidelb). 2023. PMID: 37052648 Review. German.
-
Surgery for lateral elbow pain.Cochrane Database Syst Rev. 2011 Mar 16;2011(3):CD003525. doi: 10.1002/14651858.CD003525.pub2. Cochrane Database Syst Rev. 2011. PMID: 21412883 Free PMC article.
References
-
- Boyd HB, McLeod AC., Jr Tennis elbow. J Bone Joint Surg Am. 1973;55:1183–1187. - PubMed
-
- Coonrad RW, Hooper WR. Tennis elbow: its course, natural history, conservative and surgical management. J Bone Joint Surg Am. 1973;55:1177–1182. - PubMed
-
- Fuselier HA, Prats L, Fontenot C, Gauthier A., Jr Comparison of mobile lithotripters at one institution: Healthtronics Lithotron, Dornier MFL-5000, and Dornier Doli. J Endourol. 1999;13:539–542. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
