

Human medial frontal cortex mediates unconscious inhibition of voluntary action
- PMID: 17553420
- PMCID: PMC1890004
- DOI: 10.1016/j.neuron.2007.05.016
Human medial frontal cortex mediates unconscious inhibition of voluntary action
Abstract
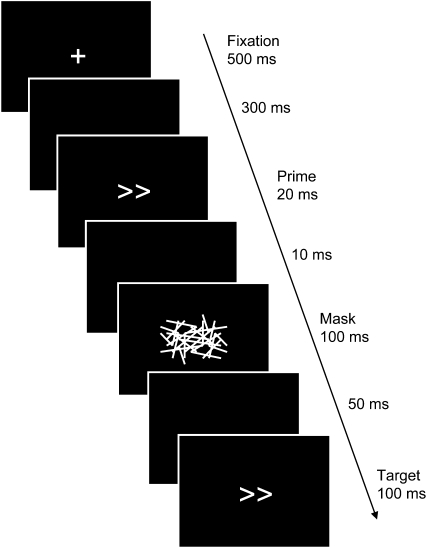
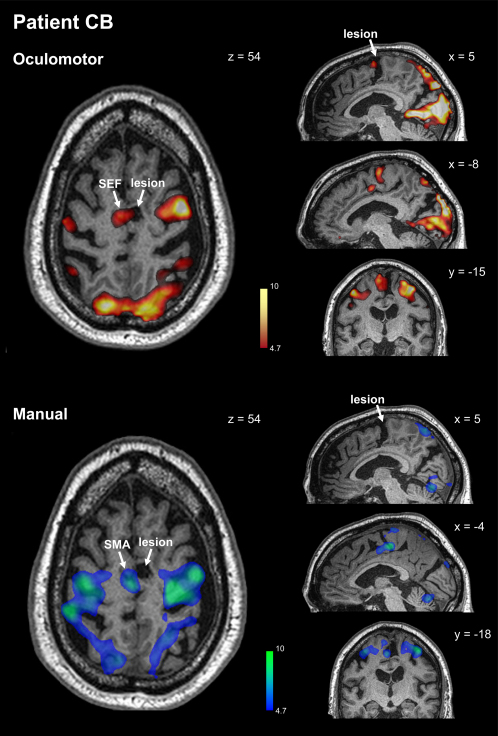
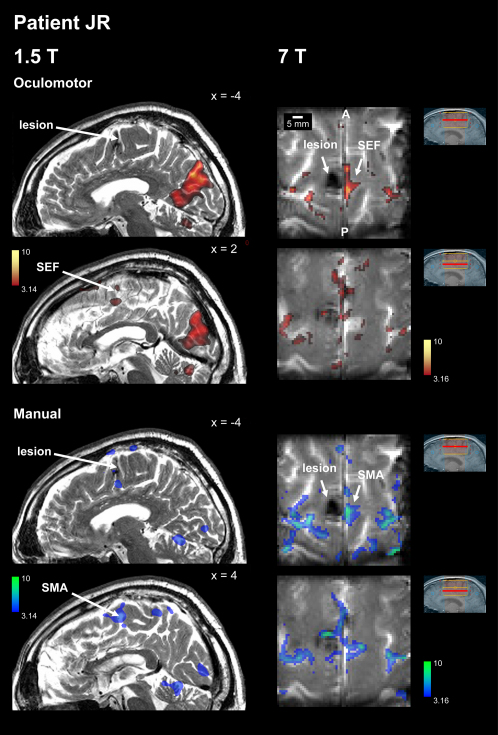
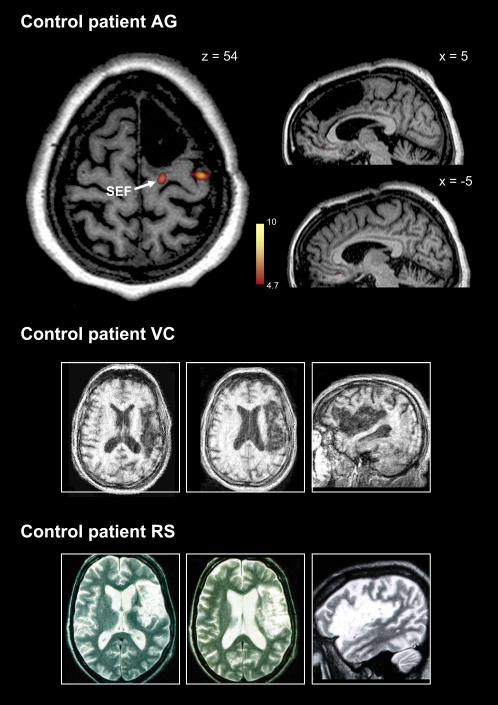
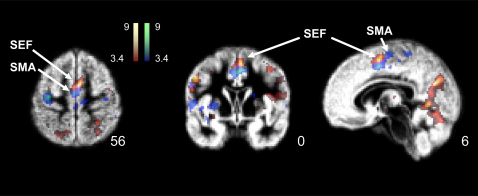
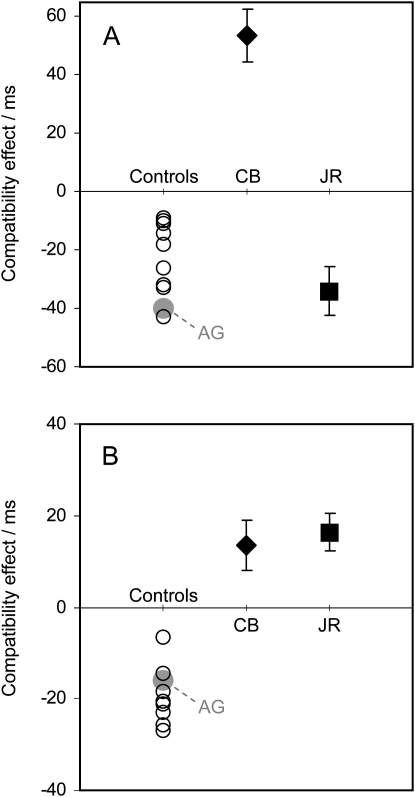
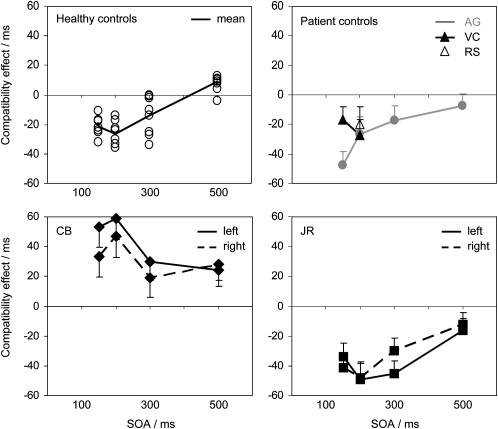
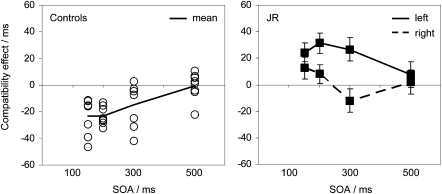
Within the medial frontal cortex, the supplementary eye field (SEF), supplementary motor area (SMA), and pre-SMA have been implicated in the control of voluntary action, especially during motor sequences or tasks involving rapid choices between competing response plans. However, the precise roles of these areas remain controversial. Here, we study two extremely rare patients with microlesions of the SEF and SMA to demonstrate that these areas are critically involved in unconscious and involuntary motor control. We employed masked-prime stimuli that evoked automatic inhibition in healthy people and control patients with lateral premotor or pre-SMA damage. In contrast, our SEF/SMA patients showed a complete reversal of the normal inhibitory effect--ocular or manual--corresponding to the functional subregion lesioned. These findings imply that the SEF and SMA mediate automatic effector-specific suppression of motor plans. This automatic mechanism may contribute to the participation of these areas in the voluntary control of action.
Figures
Comment in
-
A paradoxical role for inhibition in initiation.Neuron. 2007 Jun 7;54(5):669-70. doi: 10.1016/j.neuron.2007.05.025. Neuron. 2007. PMID: 17553416 Review.
References
-
- Amador N., Schlag-Rey M., Schlag J. Primate antisaccade. II. Supplementary eye field neuronal activity predicts correct performance. J. Neurophysiol. 2004;91:1672–1689. - PubMed
-
- Chainay H., Krainik A., Tanguy M.L., Gerardin E., Le Bihan D., Lehericy S. Foot, face and hand representation in the human supplementary motor area. Neuroreport. 2004;15:765–769. - PubMed
-
- Chen L.L., Wise S.P. Neuronal-activity in the supplementary eye field during acquisition of conditional oculomotor associations. J. Neurophysiol. 1995;73:1101–1121. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
