

Developments in post-marketing comparative effectiveness research
- PMID: 17554243
- PMCID: PMC2905665
- DOI: 10.1038/sj.clpt.6100249
Developments in post-marketing comparative effectiveness research
Abstract
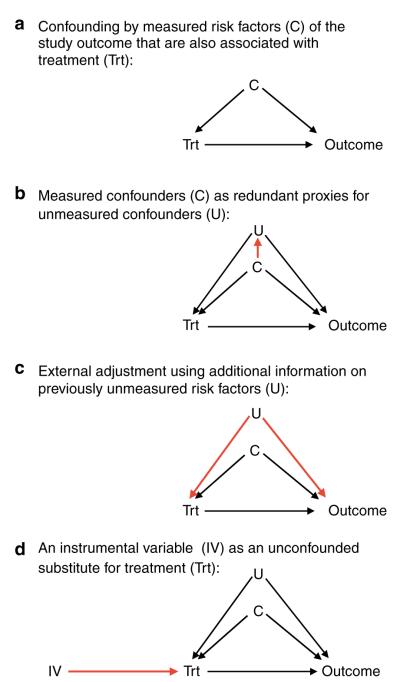
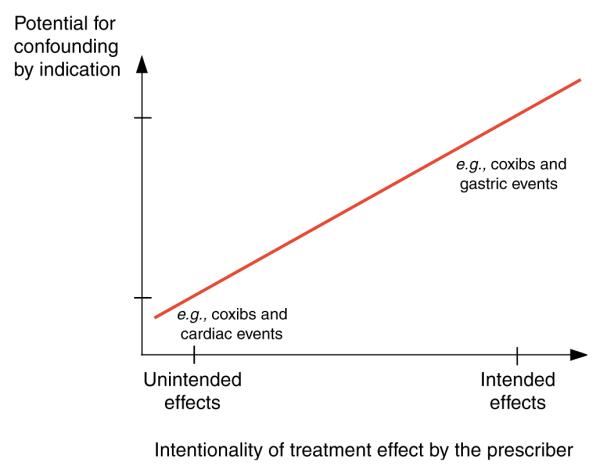
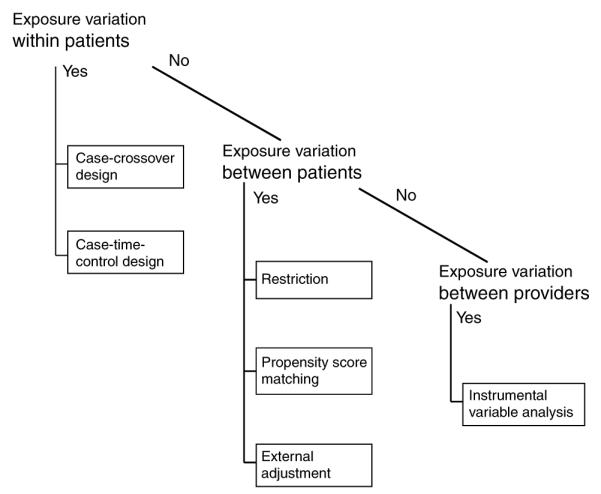
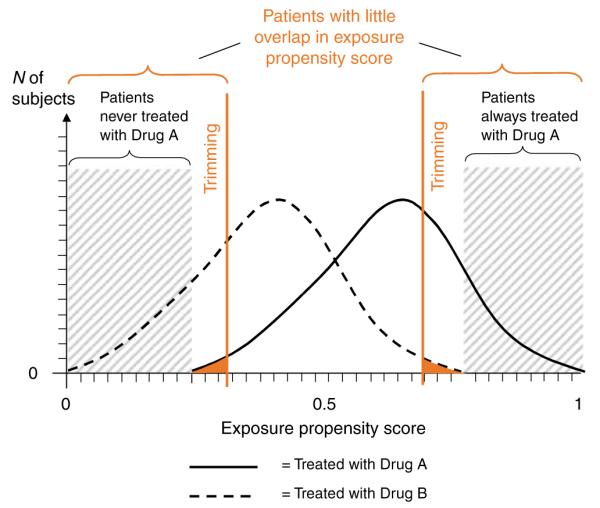
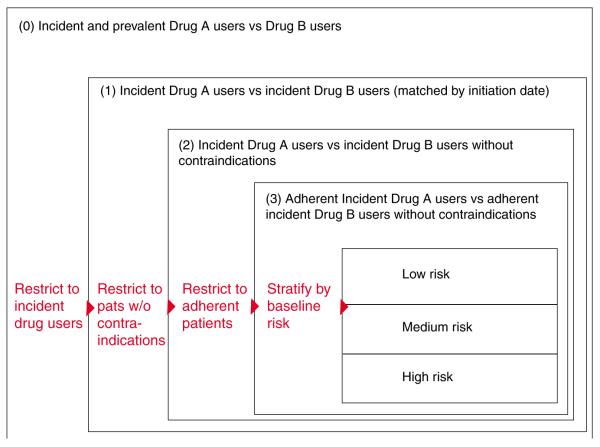
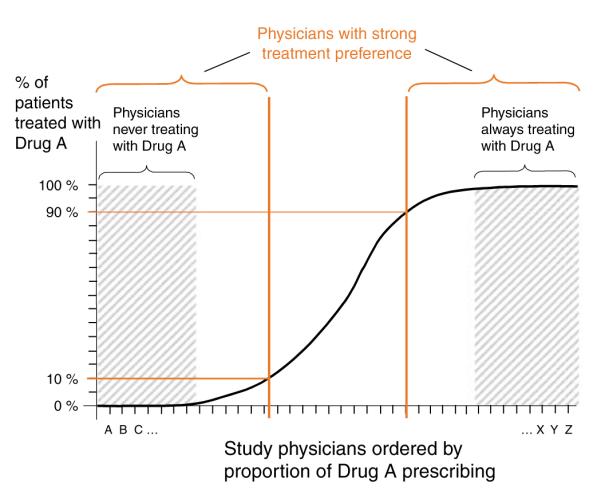
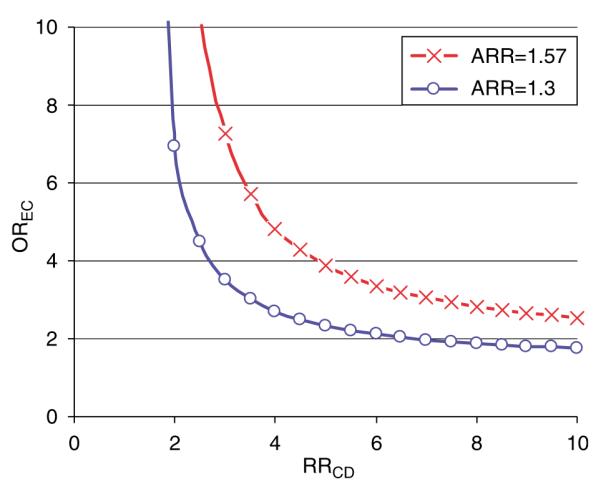
Physicians and insurers need to weigh the effectiveness of new drugs against existing therapeutics in routine care to make decisions about treatment and formularies. Because Food and Drug Administration (FDA) approval of most new drugs requires demonstrating efficacy and safety against placebo, there is limited interest by manufacturers in conducting such head-to-head trials. Comparative effectiveness research seeks to provide head-to-head comparisons of treatment outcomes in routine care. Health-care utilization databases record drug use and selected health outcomes for large populations in a timely way and reflect routine care, and therefore may be the preferred data source for comparative effectiveness research. Confounding caused by selective prescribing based on indication, severity, and prognosis threatens the validity of non-randomized database studies that often have limited details on clinical information. Several recent developments may bring the field closer to acceptable validity, including approaches that exploit the concepts of proxy variables using high-dimensional propensity scores, within-patient variation of drug exposure using crossover designs, and between-provider variation in prescribing preference using instrumental variable (IV) analyses.
Figures
References
-
- Cochrane A. Effectiveness and Efficiency: Random Reflection on Health Services. Nuffiled Provincial Trust; London: 1972.
-
- Pisano DJ, Mantus D. FDA Regulatory Affairs: A Guide for Prescription Drugs, Medical Devices, and Biologics. CRC Press; Boca Rotan, FL: 2004.
-
- Bucher HC, Guyatt GH, Griffith LE, Walter SD. The results of direct and indirect treatment comparisons in meta-analysis of randomized controlled trials. J. Clin. Epidemiol. 1997;50:683–691. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
