

Knee instability after acute ACL rupture affects movement patterns during the mid-stance phase of gait
- PMID: 17557321
- PMCID: PMC2859715
- DOI: 10.1002/jor.20440
Knee instability after acute ACL rupture affects movement patterns during the mid-stance phase of gait
Abstract
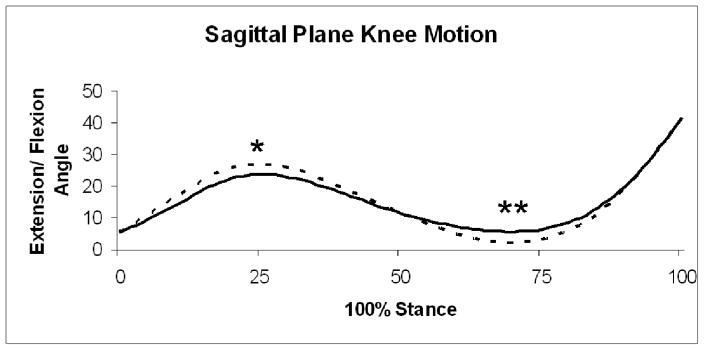
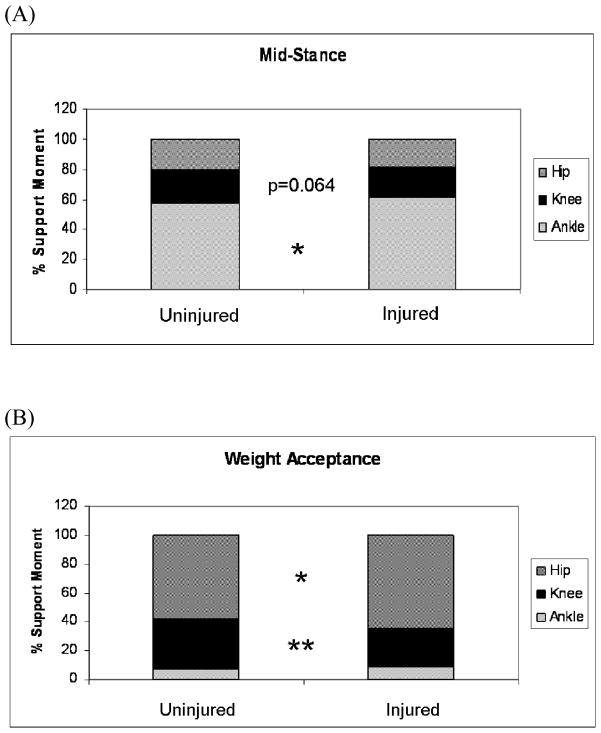
The purpose of this study was to identify gait asymmetries during the mid-stance phase of gait among subjects with knee instability ("non-copers") after acute anterior cruciate ligament (ACL) rupture. Twenty-one non-copers with acute, isolated ACL injury ambulated at their intentional walking speed as kinetic, kinematic, and electromyographic (EMG) data were collected bilaterally. Lower extremity movement patterns and muscle activity were analyzed during the mid-stance and weight acceptance phases of stance. When compared to the uninjured limb, subjects exhibited lower sagittal plane knee excursions and peak knee angles, and higher muscle co-contraction on the injured limb. There was a lower knee flexion moment at peak knee extension, a trend for the knee contribution to the total support moment to be lower, and a higher ankle contribution to the total support moment on the injured limb. There were differences in the magnitude of muscle activity which included higher hamstring activity and lower soleus activity on the injured limb. Changes in quadriceps, soleus, and hamstring muscle activity on the injured limb were identified during weight acceptance that had not previously been reported, while hip compensation for a lower knee contribution to the total support moment has been described. Non-copers consistently stabilize their knee with a stiffening strategy involving less knee motion and higher muscle contraction. The variable combination of muscle adaptations that produce joint stiffness, and the ability of both the ankle and the hip to compensate for lower knee control indicate the non-coper neuromuscular system may be more malleable than previously believed.
Figures


Similar articles
-
Gait and neuromuscular asymmetries after acute anterior cruciate ligament rupture.Med Sci Sports Exerc. 2012 Aug;44(8):1490-6. doi: 10.1249/MSS.0b013e31824d2783. Med Sci Sports Exerc. 2012. PMID: 22330021 Free PMC article.
-
Evaluation of the walking pattern in two types of patients with anterior cruciate ligament deficiency: copers and non-copers.Eur J Appl Physiol. 2003 May;89(3-4):301-8. doi: 10.1007/s00421-002-0787-x. Epub 2003 Mar 14. Eur J Appl Physiol. 2003. PMID: 12736838 Clinical Trial.
-
Elucidation of a potentially destabilizing control strategy in ACL deficient non-copers.J Electromyogr Kinesiol. 2005 Feb;15(1):83-92. doi: 10.1016/j.jelekin.2004.07.003. J Electromyogr Kinesiol. 2005. PMID: 15642656
-
Contributions to the understanding of gait control.Dan Med J. 2014 Apr;61(4):B4823. Dan Med J. 2014. PMID: 24814597 Review.
-
Progressive Changes in Walking Kinematics and Kinetics After Anterior Cruciate Ligament Injury and Reconstruction: A Review and Meta-Analysis.J Athl Train. 2017 Sep;52(9):847-860. doi: 10.4085/1062-6050-52.6.06. J Athl Train. 2017. PMID: 28985125 Free PMC article. Review.
Cited by
-
The mental representation of the human gait in young and older adults.Front Psychol. 2015 Jul 14;6:943. doi: 10.3389/fpsyg.2015.00943. eCollection 2015. Front Psychol. 2015. PMID: 26236249 Free PMC article.
-
Association between long-term quadriceps weakness and early walking muscle co-contraction after total knee arthroplasty.Knee. 2013 Dec;20(6):426-31. doi: 10.1016/j.knee.2012.12.008. Epub 2013 Jan 23. Knee. 2013. PMID: 23352711 Free PMC article.
-
Altered gait characteristics in individuals with knee osteoarthritis and self-reported knee instability.J Orthop Sports Phys Ther. 2015 May;45(5):351-9. doi: 10.2519/jospt.2015.5540. Epub 2015 Mar 26. J Orthop Sports Phys Ther. 2015. PMID: 25808531 Free PMC article. Clinical Trial.
-
Anterior Cruciate Ligament Injury: Compensation during Gait using Hamstring Muscle Activity.Open Biomed Eng J. 2010 Jun 10;4:99-106. doi: 10.2174/1874120701004010099. Open Biomed Eng J. 2010. PMID: 20721326 Free PMC article.
-
Gait deviations of patients with ruptured anterior cruciate ligament: a cross-sectional gait analysis study on male patients.Knee Surg Relat Res. 2021 Dec 24;33(1):45. doi: 10.1186/s43019-021-00128-w. Knee Surg Relat Res. 2021. PMID: 34952655 Free PMC article. No abstract available.
References
-
- Rudolph KS, Axe MJ, Buchanan TS, et al. Dynamic stability in the anterior cruciate ligament deficient knee. Knee Surg Sports Traumatol Arthrosc. 2001;9:62–71. - PubMed
-
- Wexler G, Hurwitz DE, Bush-Joseph CA, et al. Functional gait adaptations in patients with anterior cruciate ligament deficiency over time. Clin Orthop Relat Res. 1998:166–75. - PubMed
-
- Teixeira da Fonseca S, Silva PL, Ocarino JM, et al. Analyses of dynamic co-contraction level in individuals with anterior cruciate ligament injury. J Electromyogr Kinesiol. 2004;14:239–47. - PubMed
-
- Berchuck M, Andriacchi TP, Bach BR, Reider B. Gait adaptations by patients who have a deficient anterior cruciate ligament. J Bone Joint Surg Am. 1990;72:871–7. - PubMed
-
- Knoll Z, Kiss RM, Kocsis L. Gait adaptation in ACL deficient patients before and after anterior cruciate ligament reconstruction surgery. J Electromyogr Kinesiol. 2004;14:287–94. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
