

The complexity of medication regimens and test ordering for patients with diabetes from 1995 to 2003
- PMID: 17559738
- PMCID: PMC2364712
- DOI: 10.1185/030079907X199600
The complexity of medication regimens and test ordering for patients with diabetes from 1995 to 2003
Abstract
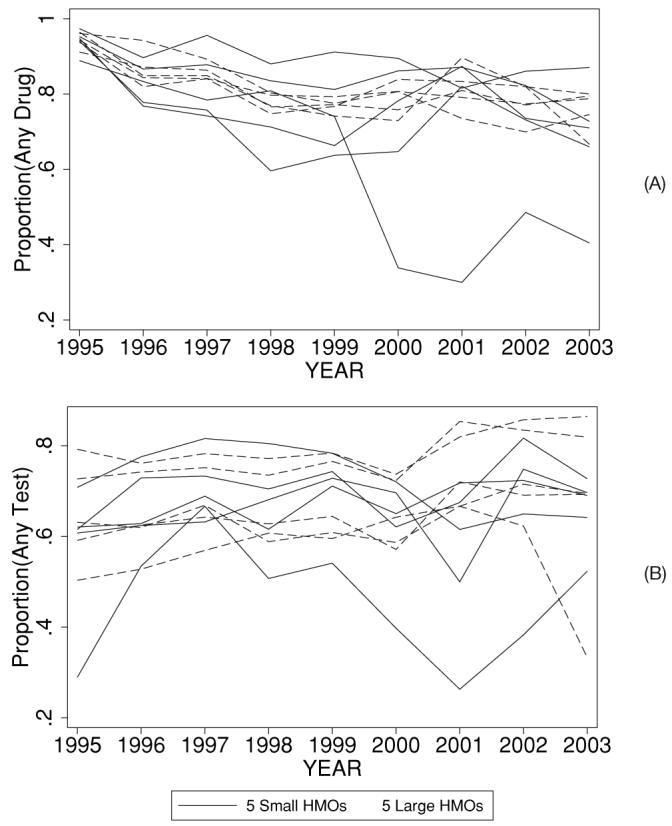
Objective: Diabetes care has become increasingly complex. We set out to quantify recent trends in the complexity of medication regimens and test ordering for diabetes patients continuously enrolled in health plans affiliated with a large, regional US health maintenance organization, with representation in the South and Midwest.
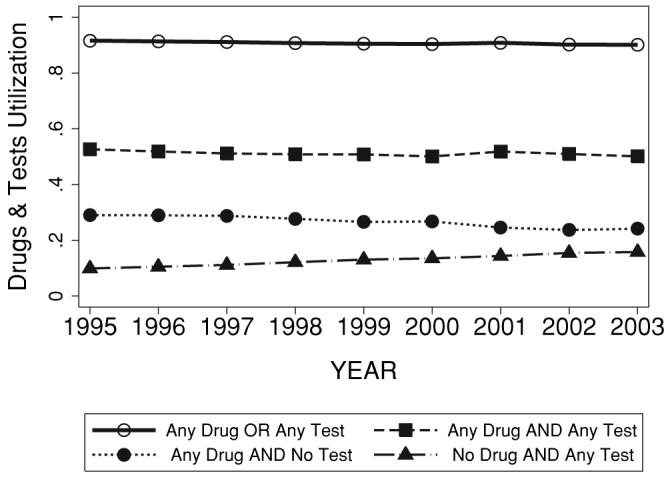
Research design and methods: We provide descriptive trends analysis of overall diabetes care complexity (number of components [i.e., glucose, blood pressure, cholesterol control], number of medications/tests) from 1995 to 2003 for adults with diabetes (N = 304,233).
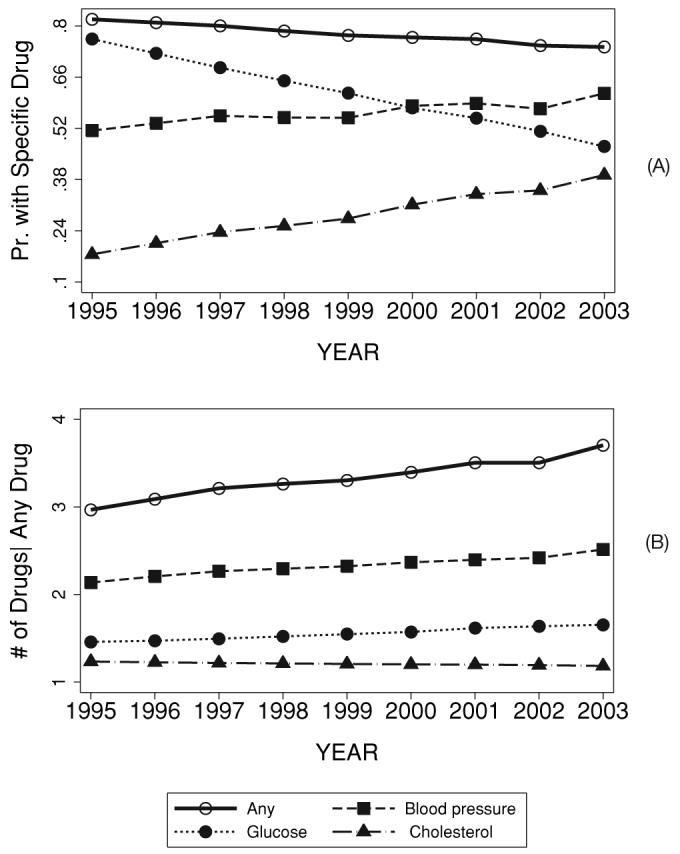
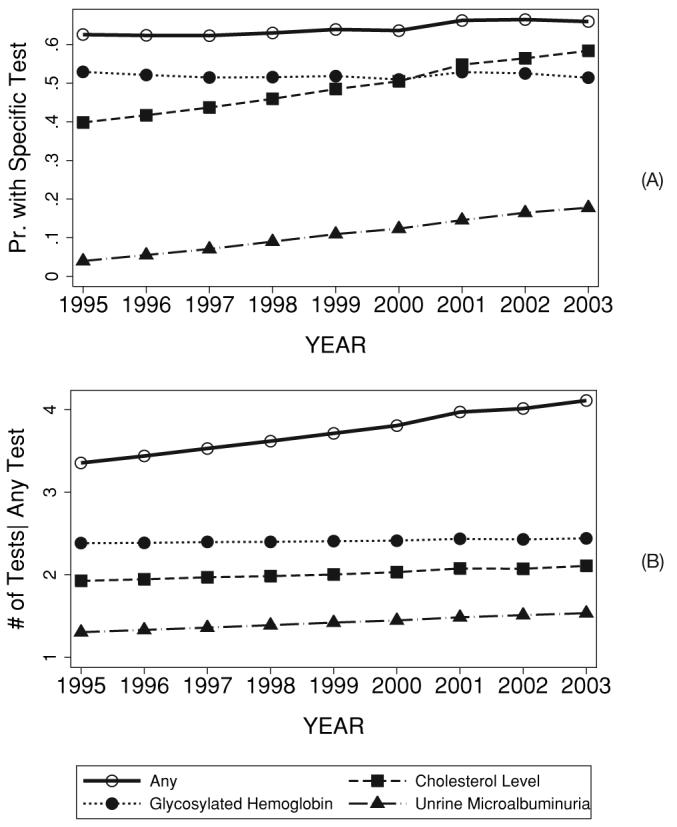
Main outcome measures: The main outcomes were (1) the proportion of patients receiving diabetes-related medications (blood glucose, blood pressure, and cholesterol control agents), (2) the average number of medications, (3) the proportion of patients receiving diabetes-related tests (glycosylated hemoglobin [HbA1c], urine microalbumin, and serum cholesterol), (4) and the average number of tests ordered within the first year that a patient had any indication of diabetes.
Results: The proportion of patients on cholesterol lowering drugs (18% --> 39%, p < 0.01) and blood pressure lowering drugs (51% --> 62%, p = 0.04) rose significantly, while the proportion on glucose lowering drugs fell (76% --> 47%, p < 0.01). Among patients prescribed medications, the average total number of diabetes-related medications rose from 2.96 to 3.70 medications (p < 0.01) with smaller increases seen for glucose lowering (1.45 --> 1.65, p < 0.01) and blood pressure lowering regimens (2.14 --> 2.51, p < 0.01), and no change for cholesterol lowering drugs (1.23 --> 1.19, p = 0.19). For laboratory tests, the proportion receiving cholesterol (40% --> 58%), and urine microalbumin (4% --> 18%) (all p's < 0.01) rose significantly, while the testing rates for HbA(1c) remained unchanged. The average total number of tests ordered per year increased significantly from 3.34 to 4.10 (p < 0.01) with more modest increases observed for individual tests.
Limitation: Trends analyses are unadjusted for many clinical characteristics that might influence the complexity of diabetes care.
Conclusions: Diabetes care grew more complex with the largest change in the number of patients receiving multi-component diabetes care. While the use of blood pressure and cholesterol lowering drugs rose overall, the proportion of patients using glucose lowering drugs declined and the average number of prescribed glucose lowering drugs did not increase in a clinically significant manner.
Figures
References
-
- UK Prospective Diabetes Study Group Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33) Lancet. 1998;352:837–53. - PubMed
-
- Pyorala K, Pedersen TR, Kjekshus J, et al. Cholesterol lowering with simvastatin improves prognosis of diabetic patients with coronary heart disease: a subgroup analysis of the Scandinavian Simvastatin Survival Study (4S) Diabetes Care. 1997;20:614–20. - PubMed
-
- Goldberg RB, Mellies MJ, Sacks FM, et al. Cardiovascular events and their reduction with pravastatin in diabetic and glucose-intolerant myocardial infarction survivors with average cholesterol levels: subgroup analyses in the Cholesterol and Recurrent Events Trial. Circulation. 1998;98:2513–9. - PubMed
-
- Gaede P, Vedel P, Larsen N, et al. Multifactorial intervention and cardiovascular disease in patients with type 2 diabetes. New Eng J Med. 2003;348:383–93. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous