

Effects of treatments for symptoms of painful diabetic neuropathy: systematic review
- PMID: 17562735
- PMCID: PMC1914460
- DOI: 10.1136/bmj.39213.565972.AE
Effects of treatments for symptoms of painful diabetic neuropathy: systematic review
Abstract
Objective: To evaluate the effects of treatments for the symptoms of painful diabetic neuropathy.
Design: Systematic review.
Data sources: Articles (English and full text) on double blind randomised trials found by searching with the key words anticonvulsant, antidepressant, non-steroidal anti-inflammatory drugs, tramadol, opioid, ion channel blocker, diabetic neuropathy, diabetic peripheral neuropathy, peripheral neuropathy, and neuropathy. The search included Medline, Embase, EMB reviews-AP Journal club, and the Cochrane central register of controlled trials.
Study selection: Randomised controlled trials comparing topically applied and orally administered drugs with a placebo in adults with painful diabetic neuropathy.
Data extraction: Data were extracted to examine quality of methods, characteristics of studies and patients, efficacy, and side effects. The primary outcome was dichotomous information for 50% or moderate reduction of pain. Secondary outcomes were 30% reduction of pain and withdrawals related to adverse events.
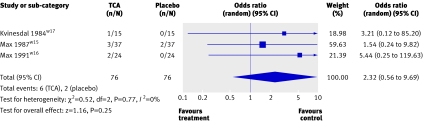
Results: Odds ratios were calculated for achievement of 30%, 50%, or moderate pain relief and for withdrawals related to adverse effects. Twenty five reports were included and seven were excluded. The 25 included reports compared anticonvulsants (n=1270), antidepressants (94), opioids (329), ion channel blockers (173), N-methyl-D-aspartate antagonist (14), duloxetine (805), capsaicin (277), and isosorbide dinitrate spray (22) with placebo. The odds ratios in terms of 50% pain relief were 5.33 (95% confidence interval 1.77 to 16.02) for traditional anticonvulsants, 3.25 (2.27 to 4.66) for newer generation anticonvulsants, and 22.24 (5.83 to 84.75) for tricylic antidepressants. The odds ratios in terms of withdrawals related to adverse events were 1.51 (0.33 to 6.96) for traditional anticonvulsants, 2.98 (1.75 to 5.07) for newer generation anticonvulsants, and 2.32 (0.59 to 9.69) for tricylic antidepressants. Insufficient dichotomous data were available to calculate the odds ratios for ion channel blockers.
Conclusion: Anticonvulsants and antidepressants are still the most commonly used options to manage diabetic neuropathy. Oral tricyclic antidepressants and traditional anticonvulsants are better for short term pain relief than newer generation anticonvulsants. Evidence of the long term effects of oral antidepressants and anticonvulsants is still lacking. Further studies are needed on opioids, N-methyl-D-aspartate antagonists, and ion channel blockers.
Conflict of interest statement
Figures















Comment in
-
Tricyclics, capsaicin, and older anticonvulsants are best for neuropathy.J Fam Pract. 2007 Oct;56(10):793. J Fam Pract. 2007. PMID: 17912780 No abstract available.
-
Review: tricyclic antidepressants, anticonvulsants, opioids, and capsaicin cream are effective treatments for diabetic neuropathy.ACP J Club. 2008 Jan-Feb;148(1):2. ACP J Club. 2008. PMID: 18170989 No abstract available.
-
Review: TCAs, anticonvulsants, opioids, and capsaicin cream are effective for diabetic neuropathy.Evid Based Med. 2008 Feb;13(1):21. doi: 10.1136/ebm.13.1.21. Evid Based Med. 2008. PMID: 18234929 No abstract available.
References
-
- Greene DA, Stevens MJ, Feldman EL. Diabetic neuropathy: scope of the syndrome. Am J Med 1999;107:2-8S. - PubMed
-
- Klein C, Polydefkis M, Chandhry V. Peripheral neuropathy treatment trials. In: Biller J, Bogousslavaky J, eds. Blue books of practical neurology: clinical trials in neurologic practice USA: Butterworth-Heinemann, 2001:261-91.
-
- Tapp RJ, Shaw JE, de Courtenm MP, Dunstan DW, Welborn TA, Zimmet PZ, et al. Foot complications in type 2 diabetes: an Australian population-based study. Diabet Med 2003;20:105-13. - PubMed
-
- Young MJ, Boulton AJM, Williams DRR, Mcleod AF, Sonksen PH. A multi-center study of the prevalence of diabetic neuropathy in patients attending UK diabetic clinics. Diabetologia 1993;36:150-4. - PubMed
-
- Fedele D, Comi G, Coscelli C, Cucinotta D, Feldman EL, Chirlanda G, et al. A multicenter study on the prevalence of diabetic neuropathy in Italy. Diabetes Care 1997;20:836-43. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical