

On the action of 5-amino-salicylic acid and sulfapyridine on M. avium including subspecies paratuberculosis
- PMID: 17565369
- PMCID: PMC1885215
- DOI: 10.1371/journal.pone.0000516
On the action of 5-amino-salicylic acid and sulfapyridine on M. avium including subspecies paratuberculosis
Abstract
Background: Introduced in 1942, sulfasalazine (a conjugate of 5-aminosalicylic acid (5-ASA) and sulfapyridine) is the most prescribed medication used to treat "inflammatory" bowel disease (IBD.) Although controversial, there are increasingly compelling data that Mycobacterium avium subspecies paratuberculosis (MAP) may be an etiological agent in some or all of IBD. We have shown that two other agents used in the therapy of IBD (methotrexate and 6-MP) profoundly inhibit MAP growth. We concluded that their most plausible mechanism of action is as antiMAP antibiotics. We herein hypothesize that the mechanism of action of 5-ASA and/or sulfapyridine may also simply be to inhibit MAP growth.
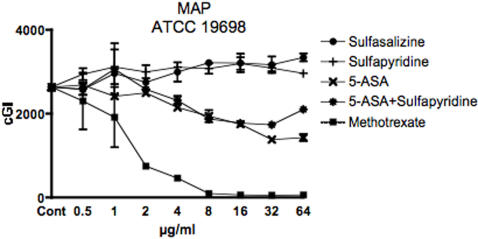
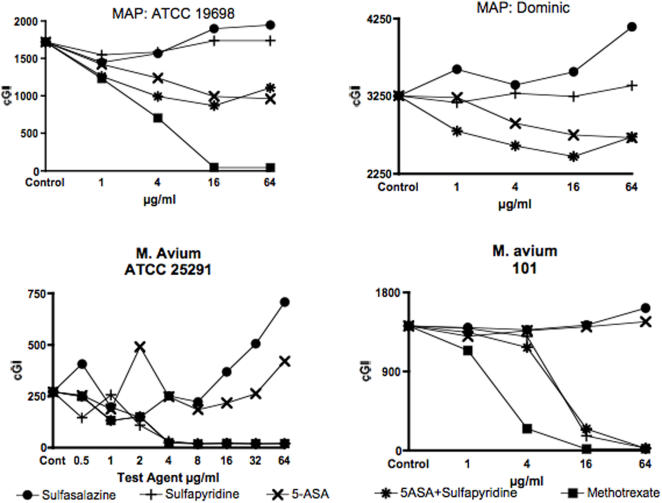
Methodology: The effect on MAP growth kinetics by sulfasalazine and its components were evaluated in bacterial culture of two strains each of MAP and M. avium, using a radiometric ((14)CO(2) BACTEC(R)) detection system that quantifies mycobacterial growth as arbitrary "growth index units" (GI). Efficacy data are presented as "percent decrease in cumulative GI" (%-DeltacGI).
Principal findings: There are disparate responses to 5-ASA and sulfapyridine in the two subspecies. Against MAP, 5-ASA is inhibitory in a dose-dependent manner (MAP ATCC 19698 46%-DeltacGI at 64 microg/ml), whereas sulfapyridine has virtually no effect. In contrast, against M. avium ATCC 25291, 5-ASA has no effect, whereas sulfapyridine (88%-DeltacGI at 4 microg/ml) is as effective as methotrexate, our positive control (88%-DeltacGI at 4 microg/ml).
Conclusions: 5-ASA inhibits MAP growth in culture. We posit that, unknowingly, the medical profession has been treating MAP infections since sulfasalazine's introduction in 1942. These observations may explain, in part, why MAP has not previously been identified as a human pathogen. We conclude that henceforth in clinical trials evaluating antiMAP agents in IBD, if considered ethical, the use of 5-ASA (as well as methotrexate and 6-MP) should be excluded from control groups.
Conflict of interest statement
Figures
References
-
- Svartz N. Salazopyrin, a new sulfanilamide preparation. A. Therapeutic Results in Rheumatic Polyarthritis. B. Therapeutic Results in Ulcerative Colitis. C. Toxic Manifestations in Treatment with Sulfanilamide Preparations. Acta Medica Scandinavica. 1942;110:577–598.
-
- Berardi RR. Inflammatory Bowel Disease. In: Herfindal ET, Gourley DR, editors. Textbook of Therapeutics Drugs and Disease Management. Baltimore: Williams and Wilkins; 1996. pp. 483–502.
-
- Green JR, Gibson JA, Kerr GD, Swarbrick ET, Lobo AJ, et al. Maintenance of remission of ulcerative colitis: a comparison between balsalazide 3 g daily and mesalazine 1.2 g daily over 12 months. ABACUS Investigator group. Aliment Pharmacol Ther. 1998;12:1207–1216. - PubMed
-
- Stenson WF, Korznik J. Inflammatory Bowel Disease. In: Yamada T, editor. Textbook of Gastroenterology. Fourth ed. Philadelphia PA.19106 USA: Lippincott Williams & Wilkins; 2003. pp. 1727–1828.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
