

Injurious mechanical ventilation in the normal lung causes a progressive pathologic change in dynamic alveolar mechanics
- PMID: 17565688
- PMCID: PMC2206429
- DOI: 10.1186/cc5940
Injurious mechanical ventilation in the normal lung causes a progressive pathologic change in dynamic alveolar mechanics
Abstract
Introduction: Acute respiratory distress syndrome causes a heterogeneous lung injury, and without protective mechanical ventilation a secondary ventilator-induced lung injury can occur. To ventilate noncompliant lung regions, high inflation pressures are required to 'pop open' the injured alveoli. The temporal impact, however, of these elevated pressures on normal alveolar mechanics (that is, the dynamic change in alveolar size and shape during ventilation) is unknown. In the present study we found that ventilating the normal lung with high peak pressure (45 cmH(2)0) and low positive end-expiratory pressure (PEEP of 3 cmH(2)O) did not initially result in altered alveolar mechanics, but alveolar instability developed over time.
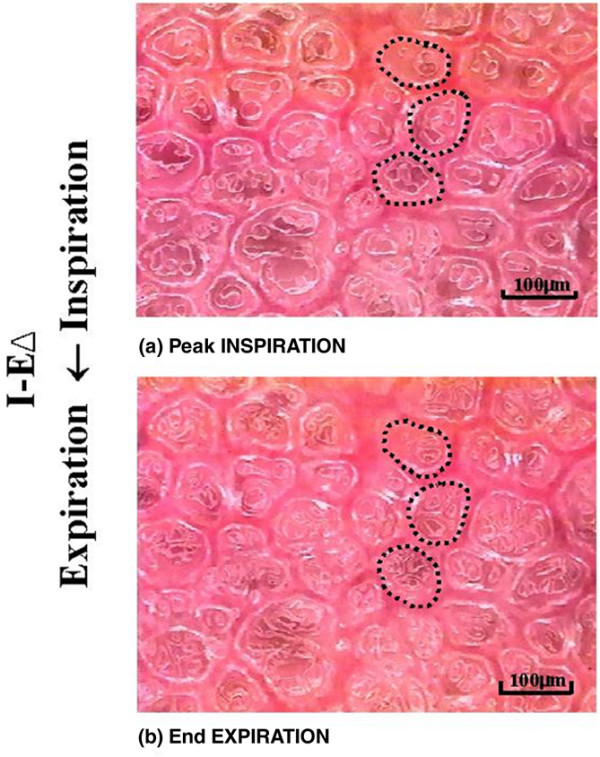
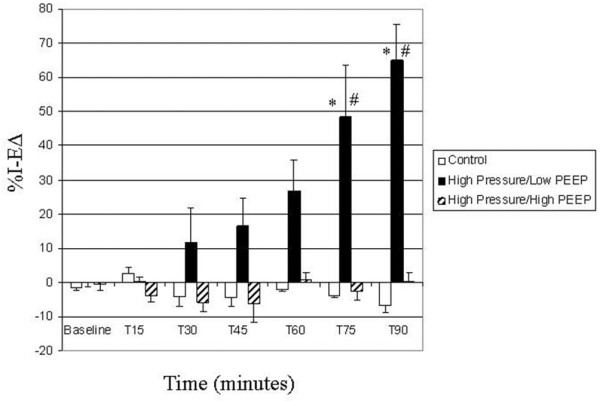
Methods: Anesthetized rats underwent tracheostomy, were placed on pressure control ventilation, and underwent sternotomy. Rats were then assigned to one of three ventilation strategies: control group (n = 3, P control = 14 cmH(2)O, PEEP = 3 cmH(2)O), high pressure/low PEEP group (n = 6, P control = 45 cmH(2)O, PEEP = 3 cmH(2)O), and high pressure/high PEEP group (n = 5, P control = 45 cmH(2)O, PEEP = 10 cmH(2)O). In vivo microscopic footage of subpleural alveolar stability (that is, recruitment/derecruitment) was taken at baseline and than every 15 minutes for 90 minutes following ventilator adjustments. Alveolar recruitment/derecruitment was determined by measuring the area of individual alveoli at peak inspiration (I) and end expiration (E) by computer image analysis. Alveolar recruitment/derecruitment was quantified by the percentage change in alveolar area during tidal ventilation (%I - E Delta).
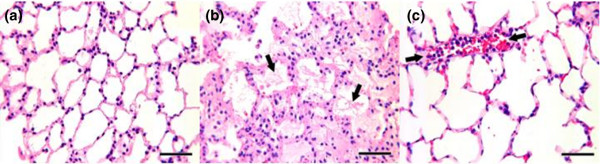
Results: Alveoli were stable in the control group for the entire experiment (low %I - E Delta). Alveoli in the high pressure/low PEEP group were initially stable (low %I - E Delta), but with time alveolar recruitment/derecruitment developed. The development of alveolar instability in the high pressure/low PEEP group was associated with histologic lung injury.
Conclusion: A large change in lung volume with each breath will, in time, lead to unstable alveoli and pulmonary damage. Reducing the change in lung volume by increasing the PEEP, even with high inflation pressure, prevents alveolar instability and reduces injury. We speculate that ventilation with large changes in lung volume over time results in surfactant deactivation, which leads to alveolar instability.
Figures

Similar articles
-
Altered alveolar mechanics in the acutely injured lung.Crit Care Med. 2001 May;29(5):1049-55. doi: 10.1097/00003246-200105000-00036. Crit Care Med. 2001. PMID: 11383531
-
Alveolar instability caused by mechanical ventilation initially damages the nondependent normal lung.Crit Care. 2007;11(5):R104. doi: 10.1186/cc6122. Crit Care. 2007. PMID: 17877789 Free PMC article.
-
Low-volume ventilation of preinjured lungs degrades lung function via stress concentration and progressive alveolar collapse.Am J Physiol Lung Cell Mol Physiol. 2024 Jul 1;327(1):L19-L39. doi: 10.1152/ajplung.00323.2023. Epub 2024 May 7. Am J Physiol Lung Cell Mol Physiol. 2024. PMID: 38712429
-
Time-Controlled Adaptive Ventilation (TCAV): a personalized strategy for lung protection.Respir Res. 2024 Jan 18;25(1):37. doi: 10.1186/s12931-023-02615-y. Respir Res. 2024. PMID: 38238778 Free PMC article. Review.
-
How respiratory system mechanics may help in minimising ventilator-induced lung injury in ARDS patients.Eur Respir J Suppl. 2003 Aug;42:15s-21s. doi: 10.1183/09031936.03.00420303. Eur Respir J Suppl. 2003. PMID: 12945996 Review.
Cited by
-
Assessment of hemodynamics, blood gases, and lung histopathology of healthy Pig model on two different mechanical ventilators.Heliyon. 2022 Sep 22;8(9):e10736. doi: 10.1016/j.heliyon.2022.e10736. eCollection 2022 Sep. Heliyon. 2022. PMID: 36164656 Free PMC article.
-
Anesthetic (r)evolution from the conventional concept to the minimally invasive techniques in thoracic surgery-narrative review.J Thorac Dis. 2022 Aug;14(8):3045-3060. doi: 10.21037/jtd-22-80. J Thorac Dis. 2022. PMID: 36071785 Free PMC article. Review.
-
A Physiologically Informed Strategy to Effectively Open, Stabilize, and Protect the Acutely Injured Lung.Front Physiol. 2020 Mar 19;11:227. doi: 10.3389/fphys.2020.00227. eCollection 2020. Front Physiol. 2020. PMID: 32265734 Free PMC article. Review.
-
The physical basis of ventilator-induced lung injury.Expert Rev Respir Med. 2010 Jun;4(3):373-85. doi: 10.1586/ers.10.28. Expert Rev Respir Med. 2010. PMID: 20524920 Free PMC article. Review.
-
The micromechanics of lung alveoli: structure and function of surfactant and tissue components.Histochem Cell Biol. 2018 Dec;150(6):661-676. doi: 10.1007/s00418-018-1747-9. Epub 2018 Nov 2. Histochem Cell Biol. 2018. PMID: 30390118 Free PMC article. Review.
References
-
- Amato MB, Barbas CS, Medeiros DM, Magaldi RB, Schettino GP, Lorenzi-Filho G, Kairalla RA, Deheinzelin D, Munoz C, Oliveira R, et al. Effect of a protective-ventilation strategy on mortality in the acute respiratory distress syndrome. N Engl J Med. 1998;338:347–354. doi: 10.1056/NEJM199802053380602. - DOI - PubMed
-
- Corbridge TC, Wood LD, Crawford GP, Chudoba MJ, Yanos J, Sznajder JI. Adverse effects of large tidal volume and low PEEP in canine acid aspiration. Am Rev Respir Dis. 1990;142:311–315. - PubMed
-
- Dreyfuss D, Saumon G. Role of tidal volume, FRC, and end-inspiratory volume in the development of pulmonary edema following mechanical ventilation. Am Rev Respir Dis. 1993;148:1194–1203. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
