

Low thoracic and lumbar burst fractures: radiographic and functional outcomes
- PMID: 17566793
- PMCID: PMC2223335
- DOI: 10.1007/s00586-007-0406-y
Low thoracic and lumbar burst fractures: radiographic and functional outcomes
Abstract
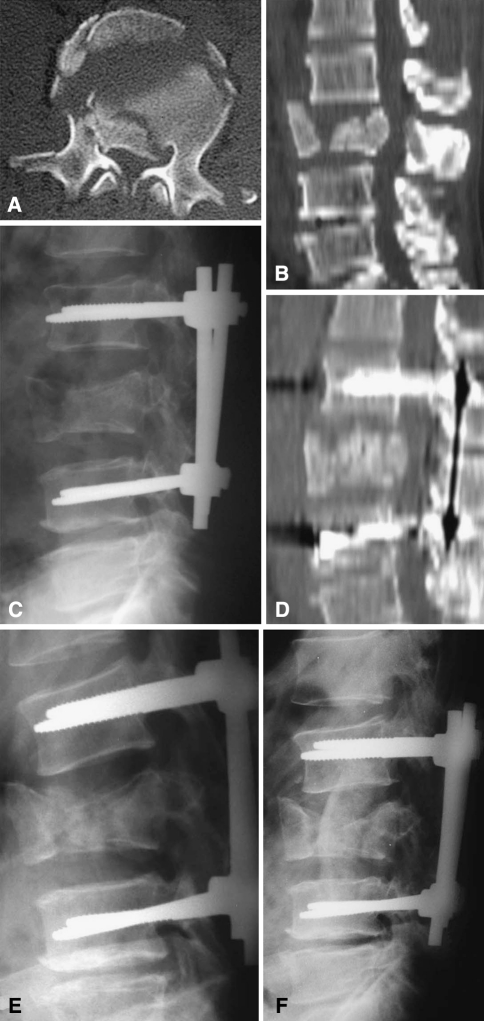
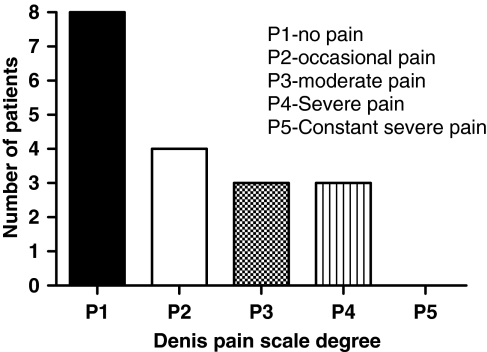
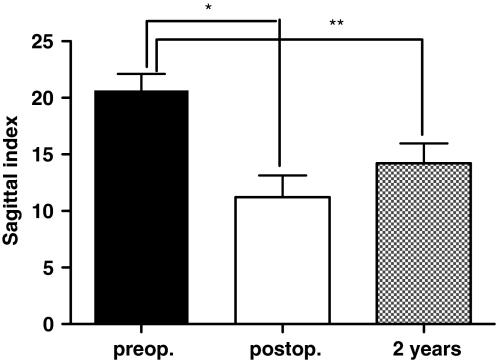
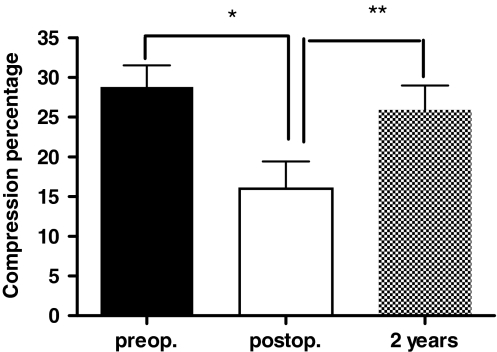
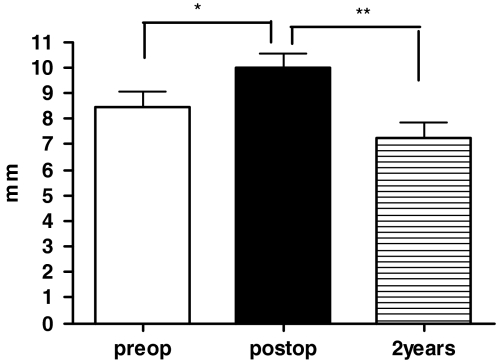
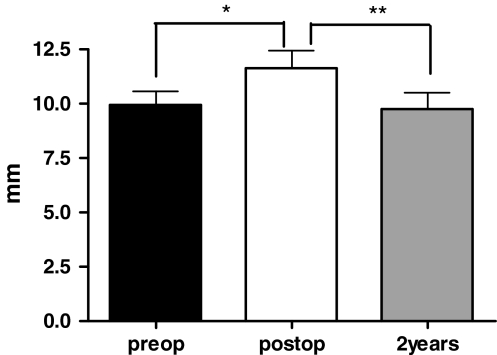
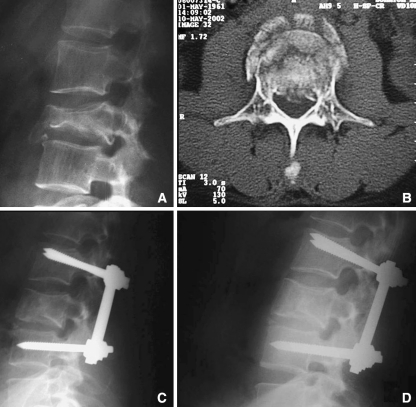
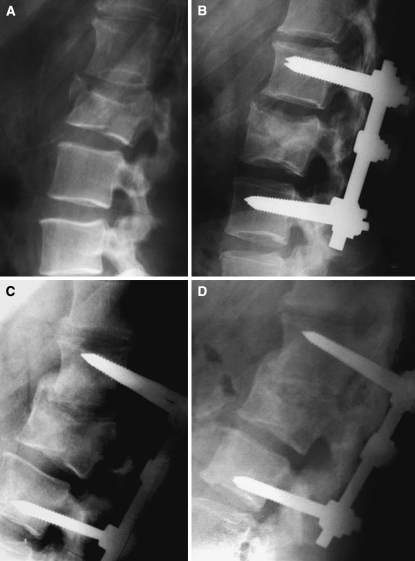
Twenty patients with thoracolumbar burst fractures (type A3 in the classification of Magerl et al.) were studied prospectively for the evaluation of clinical, radiographic and functional results. The patients were submitted to surgical treatment by posterior arthrodesis, posterior fixation and autologous transpedicular graft. The patients were followed up for 2 years after surgery and assessed on the basis of clinical (pain, neurologic deficit, postoperative infection), radiographic (load sharing classification, Farcy s sagittal index of the fractured segment, relation between traumatic vertebral body height and the adjacent vertebrae (compression percentage), height of the intervertebral disk proximal and distal to the fractured vertebra, rupture or loosening of the implants) and functional (return to work, SF-36) criteria. Two patients presented a marked loss of correction and required the placement of an anterior support graft. Pain assessment revealed that eight patients (44%) had no pain; four (22%) had occasional pain, three (17%) moderate pain, and three (17%) severe pain. According to the classification of Frankel et al., 17 patients persisted as Frankel E and one patient presented improvement of one degree, becoming Frankel D. The mean value of Farcy s sagittal index of the injured vertebral segment was 20.67 degrees +/- 6.15 degrees (range 8 degrees -32 degrees ) during the preoperative period, 11.22 degrees +/- 8.09 degrees (range -5 degrees to 21 degrees ) during the immediate postoperative period, and 14.22 degrees +/- 7.37 degrees (range 3 degrees -25 degrees ) at late evaluation. There was a statistically significant difference between the immediate postoperative values and the preoperative and late postoperative values. The compression percentage of the fractured vertebral body ranged from 9.1 to 60 (mean 28.81 +/- 11.51) during the preoperative period, from 0 to 60 (mean: 15.59 +/- 14.49) during the immediate postoperative period, and from 8 to 60 (mean: 25.9 +/- 13.02) at late evaluation. There was a statistically significant difference between the preoperative and postoperative values and between the postoperative and late postoperative values. The height of the proximal intervertebral disk ranged from 6 to 14 mm (mean 8.44 +/- 2.66) during the preoperative period, from 6 to 15 mm (mean 10 +/- 2.30) during the immediate postoperative period, and from 0 to 11 mm (mean 7.22 +/- 2.55) during the late postoperative period. A significant difference was observed between the immediate postoperative values and the preoperative and late postoperative values. The height of the intervertebral disk distal to the fractured vertebra ranged from 7 to 16 mm (mean 9.94 +/- 2.64) during the preoperative period, from 5 to 18 mm (mean 11.61 +/- 3.29) during the immediate postoperative period, and from 2 to 14 mm (mean 9.72 +/- 3.17) during the late postoperative period. There was a significant difference between the immediate postoperative values and the preoperative and late postoperative values. Except for the height of the intervertebral disk proximal to the fractured vertebra, no correlation was detected between the clinical, functional and radiologic results. The results observed in the present study indicate that other, still incompletely defined parameters influence the functional result of thoracolumbar burst fractures.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
