

Automated real time constant-specificity surveillance for disease outbreaks
- PMID: 17567912
- PMCID: PMC1919360
- DOI: 10.1186/1472-6947-7-15
Automated real time constant-specificity surveillance for disease outbreaks
Abstract
Background: For real time surveillance, detection of abnormal disease patterns is based on a difference between patterns observed, and those predicted by models of historical data. The usefulness of outbreak detection strategies depends on their specificity; the false alarm rate affects the interpretation of alarms.
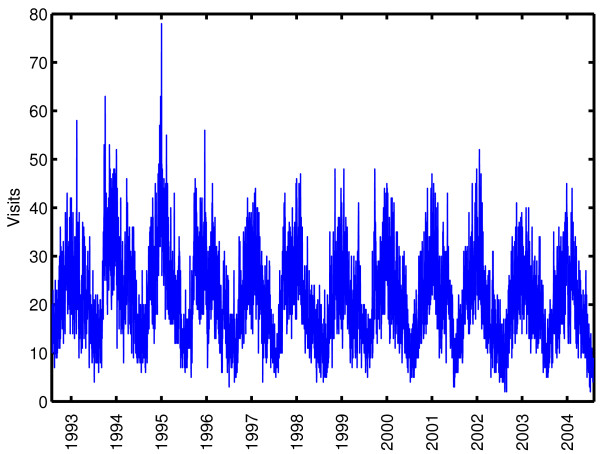
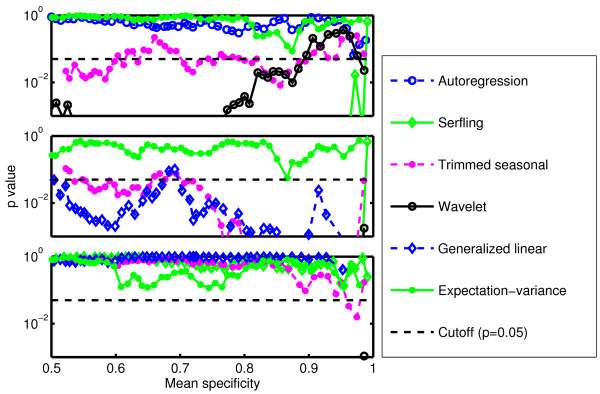
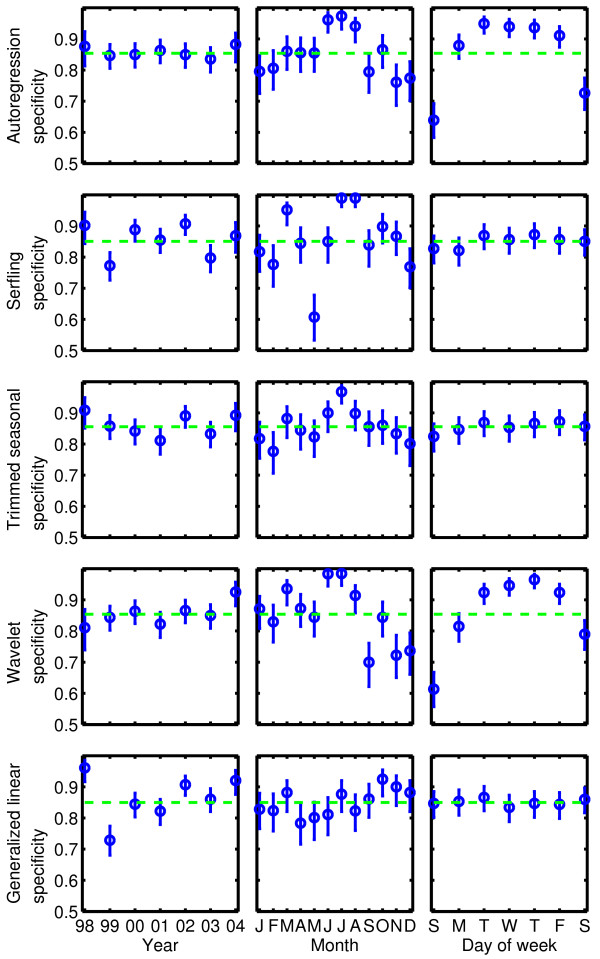
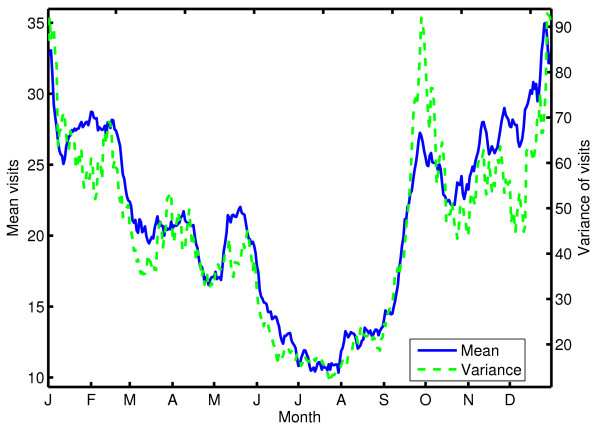
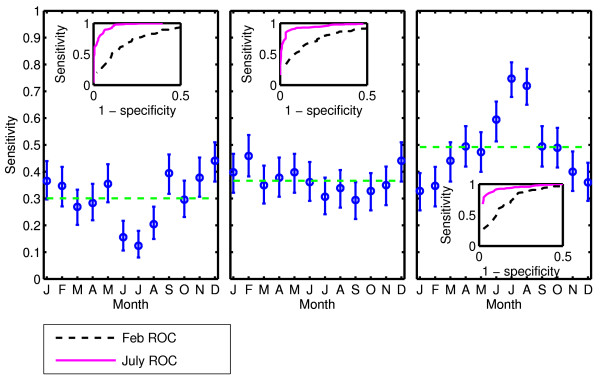
Results: We evaluate the specificity of five traditional models: autoregressive, Serfling, trimmed seasonal, wavelet-based, and generalized linear. We apply each to 12 years of emergency department visits for respiratory infection syndromes at a pediatric hospital, finding that the specificity of the five models was almost always a non-constant function of the day of the week, month, and year of the study (p < 0.05). We develop an outbreak detection method, called the expectation-variance model, based on generalized additive modeling to achieve a constant specificity by accounting for not only the expected number of visits, but also the variance of the number of visits. The expectation-variance model achieves constant specificity on all three time scales, as well as earlier detection and improved sensitivity compared to traditional methods in most circumstances.
Conclusion: Modeling the variance of visit patterns enables real-time detection with known, constant specificity at all times. With constant specificity, public health practitioners can better interpret the alarms and better evaluate the cost-effectiveness of surveillance systems.
Figures
References
-
- Yuan CM, Love S, Wilson M. Syndromic surveillance at hospital emergency departments – Southeastern Virginia. MMWR Morb Mortal Wkly Rep. 2004;53:56–58. - PubMed
-
- Heffernan R, Mostashari F, Das D, Besculides M, Rodriguez C, Greenko J, Steiner-Sichel L, Balter S, Karpati A, Thomas P, Phillips M, Ackelsberg J, Lee E, Leng J, Hartman J, Metzger K, Rosselli R, Weiss D. New York City Syndromic Surveillance Systems. MMWR Morb Mortal Wkly Rep. 2004;53:23–27. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
