

Abdominal compartment syndrome
- PMID: 17568172
- PMCID: PMC6077087
- DOI: 10.5144/0256-4947.2007.183
Abdominal compartment syndrome
Abstract
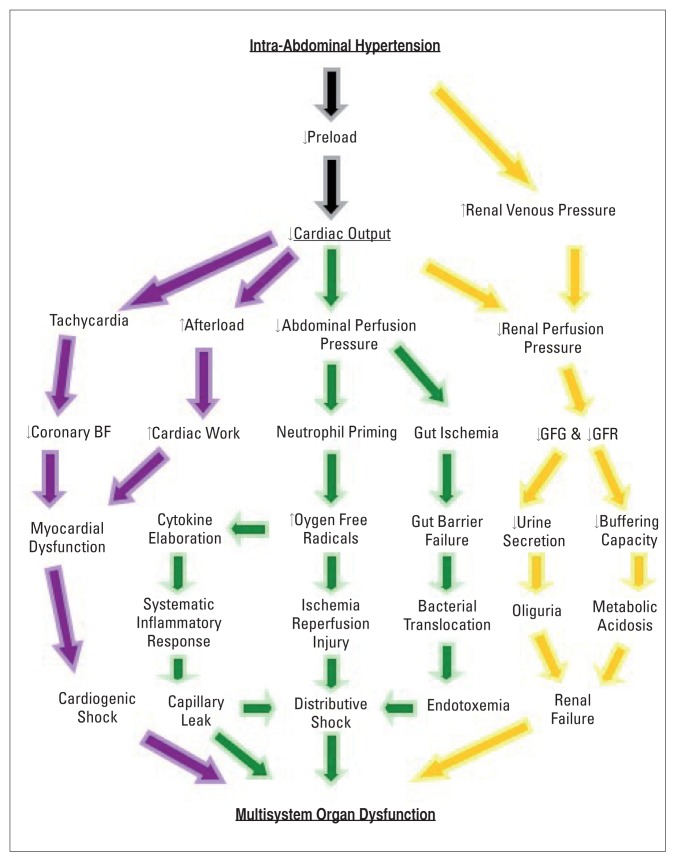
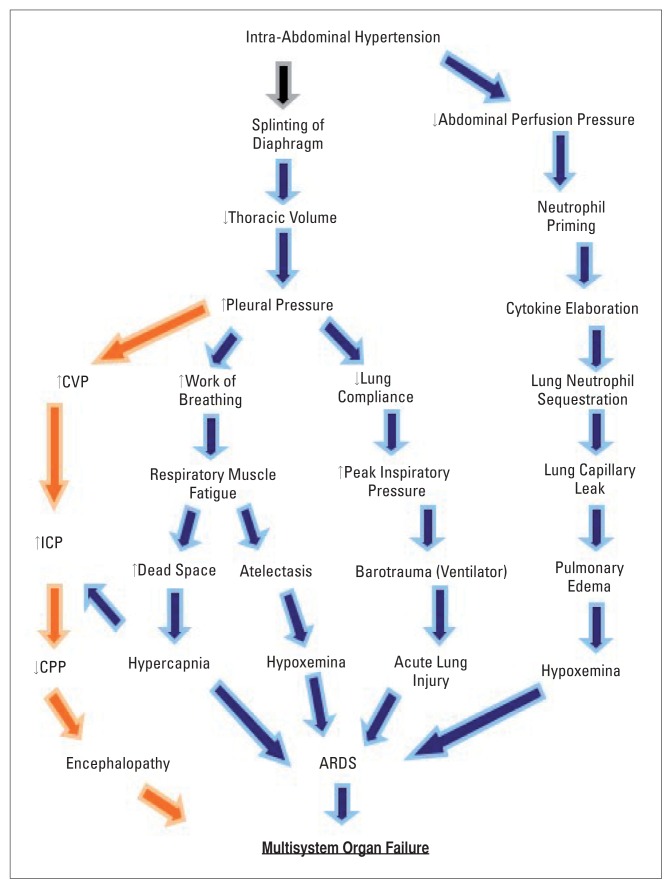
The term abdominal compartment syndrome (ACS) describes the clinical manifestations of the pathologic elevation of the intra-abdominal pressure (IAP). When the IAP exceeds 12 mm Hg it is referred to as intra-abdominal hypertension (IAH) while ACS generally sets in at an IAP in excess of 20 mm Hg. This syndrome is most commonly observed in the setting of severe abdominal trauma and in the aftermath of major abdominal operations. ACS affects mainly the respiratory, cardiovascular, renal, gastrointestinal and the central nervous systems. Fundamental to the development of ACS are the obstruction of venous return to the heart via the inferior vena cava and the splinting of the diaphragm due to elevated IAP. Preventing ACS by the identification of patients at risk and early diagnosis is paramount to its successful management. To this end a high index of suspicion is sine qua non. The management of established ACS requires clinical astuteness and decisiveness with a readily available and generous team support. The purpose of this review is to enhance awareness among clinicians about a subtle condition with a devastating impact on morbidity and mortality if undiagnosed.
Figures
References
-
- Malbrain MLNG, De Laet I, Cheatham M. Consensus Conference Definitions and Recommendations on intra-abdominal hypertension (IAH) and the Abdominal Compartment Syndrome (ACS) - the long road to the final publications, how did we get there? Acta Clinica Belgica. 2007;62(supplement 1):44–59. - PubMed
-
- Hunter JD, Damani Z. Intra-abdominal hypertension and the abdominal compartment syndrome. Anaesthesia. 2004 Sep;59(9):899–907. - PubMed
-
- Moore AF, Hargest R, Martin M, Delicata RJ. Intra-abdominal hypertension and the abdominal compartment syndrome. Br J Surg. 2004 Sep;91(9):1102–10. - PubMed
-
- Schein M. Abdominal Compartment Syndrome: Historical Background. In: Ivatury RR, Cheatham ML, Malbrain MLNG, Sugrue M, editors. Abdominal Compartment Syndrome. Landes Bioscience; 2006. pp. 1–7.
-
- Emerson H. Intra-Abdominal pressures. Arch Intern Med. 1911;7:754–784.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials