

Ten years' experience with year-round active surveillance of up to 19 respiratory pathogens in children
- PMID: 17569085
- PMCID: PMC7087302
- DOI: 10.1007/s00431-007-0496-x
Ten years' experience with year-round active surveillance of up to 19 respiratory pathogens in children
Abstract
Introduction: Surveillance systems for acute respiratory infections (ARI) in children currently are often limited in terms of the panel of pathogens and the age range investigated or are only syndromic and at times only active in the winter season.
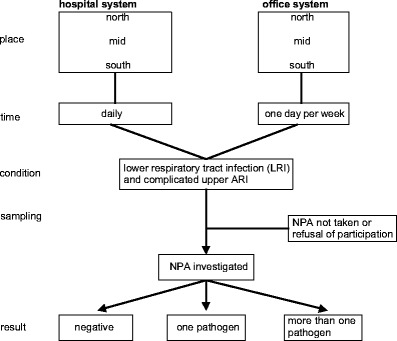
Methods: Within PID-ARI.net, a research network for ARI in children in Germany, an active, year-round surveillance system was formed in three regions from north to south for population-based analysis. Children from birth to 16 years of age were included and up to 19 noncolonizing airway pathogens were tested for with multiplex RT-PCR.
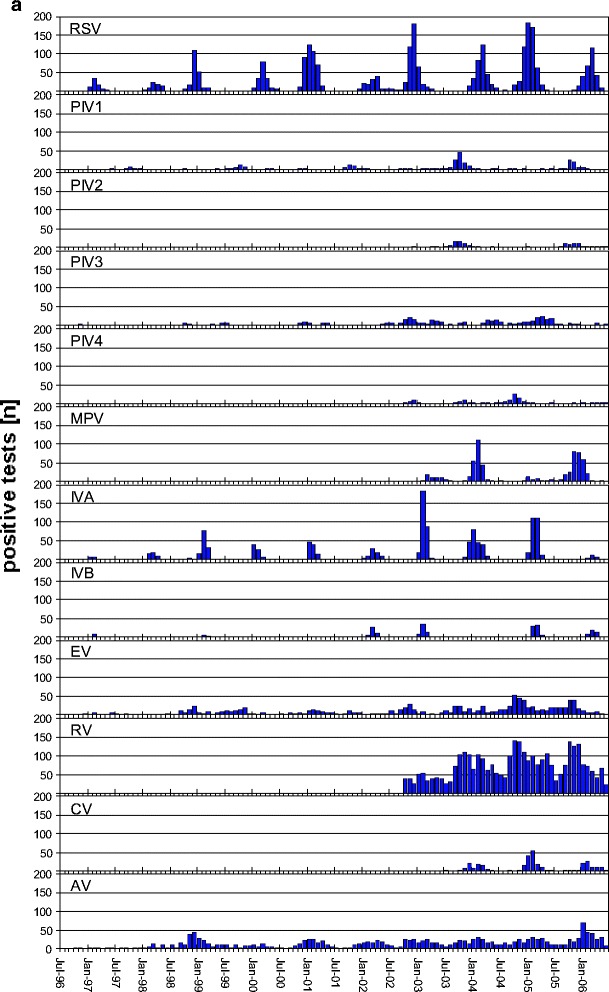
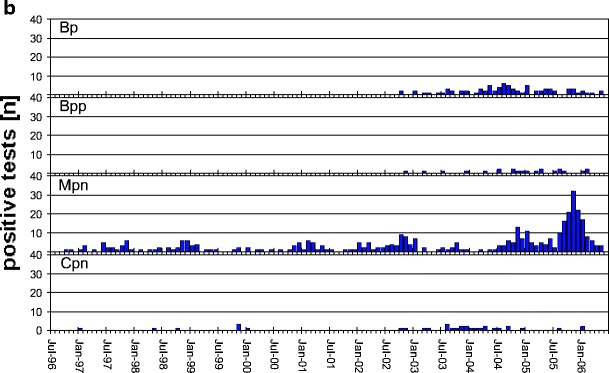
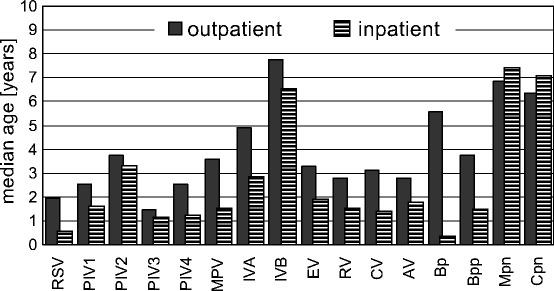
Results: In the 10-year period from July 1996 to June 2006, a total of 18,899 samples were tested. The positive rate increased with the size of the test panel to up to 72.9%. Picornaviruses (35-39%), paramyxoviruses (23-28%) and orthomyxoviruses (5.8-12.5%) comprised the highest fraction. Reoviruses and Legionella pneumophila were not found at all and Chlamydia pneumoniae and Bordetella parapertussis only rarely. Respiratory syncytial virus and parainfluenza virus (PIV) type 3 were anticyclical in rhythmicity with metapneumovirus and PIV1 and PIV2. The age medians per pathogen depended predominantly upon the attack rate and interepidemic intervals.
Conclusion: Active surveillance systems for ARI are superior to passive systems. They should be pathogen-specific and comprehensive for viruses and bacteria and age ranges. They should be population-based and multilevel to avoid bias. The impact of atypical bacteria in children was highly overestimated in earlier studies.
Figures
References
-
- Florman AL, McLean LC. The effect of altitude and weather on the occurrence of outbreaks of respiratory syncytial virus infections. J Infect Dis. 1988;158:1401–1402. - PubMed
-
- Graham NMH. Respiratory infections. In: Pless IB, editor. The epidemiology of childhood disorders. New York: Oxford University Press; 1994. pp. 173–210.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
