

Imaging findings of bisphosphonate-associated osteonecrosis of the jaws
- PMID: 17569974
- PMCID: PMC8134141
- DOI: 10.3174/ajnr.A0518
Imaging findings of bisphosphonate-associated osteonecrosis of the jaws
Abstract
Background and purpose: Bisphosphonates are drugs that decrease bone turnover by inhibiting osteoclast activity. An association between the use of bisphosphonates and osteonecrosis of the maxilla and mandible has recently been described. This study describes the imaging findings of bisphosphonate-associated osteonecrosis of the jaws.
Materials and methods: This is a retrospective series of 15 clinically diagnosed patients, identified at 3 centers. Eleven patients were women, of whom 6 had breast cancer, 3 had osteoporosis, and 2 had multiple myeloma. Of the 4 male patients, 2 had prostate cancer, 1 had multiple myeloma, and 1 had osteoporosis. The age range of the patients was 52-85 years (average, 68 years). The mandible was the clinical site of involvement in 11 patients, and the maxilla was involved in 4 patients. Imaging consisted of orthopantomograms in 14 patients, CT scans in 5 patients, and radionuclide bone scan in 1 patient. Nine patients had sequential imaging. Two radiologists reviewed the images.
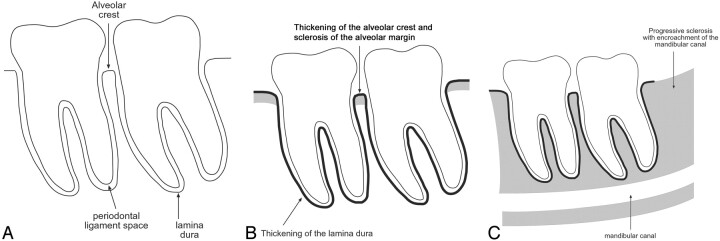
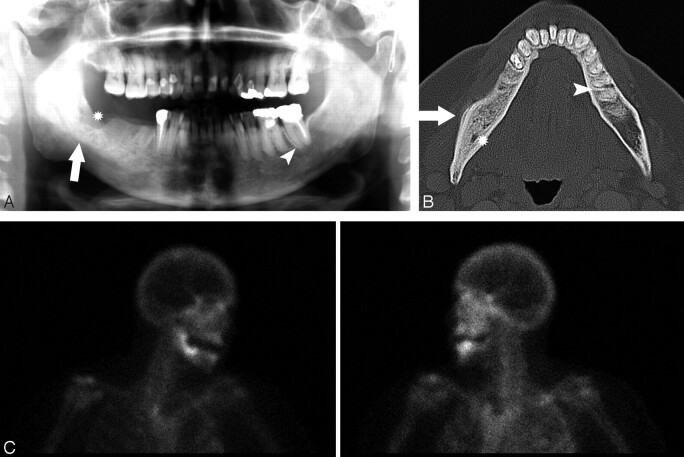
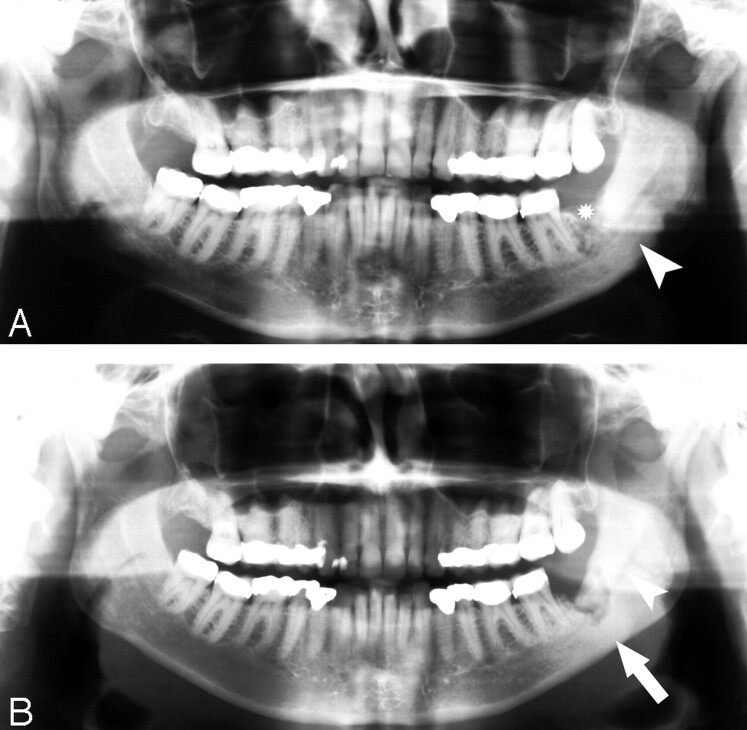
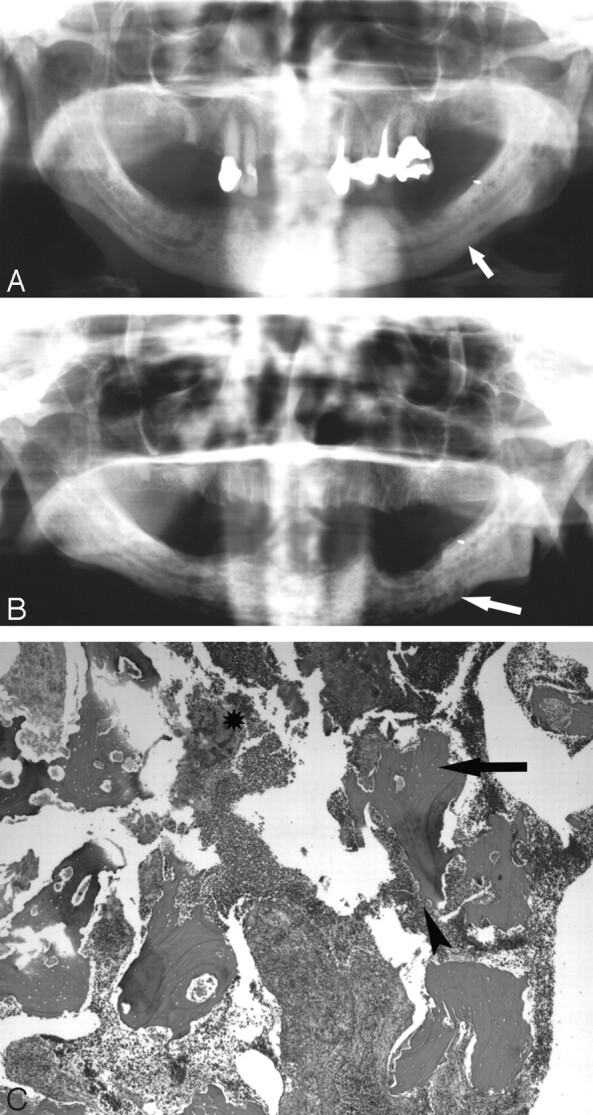
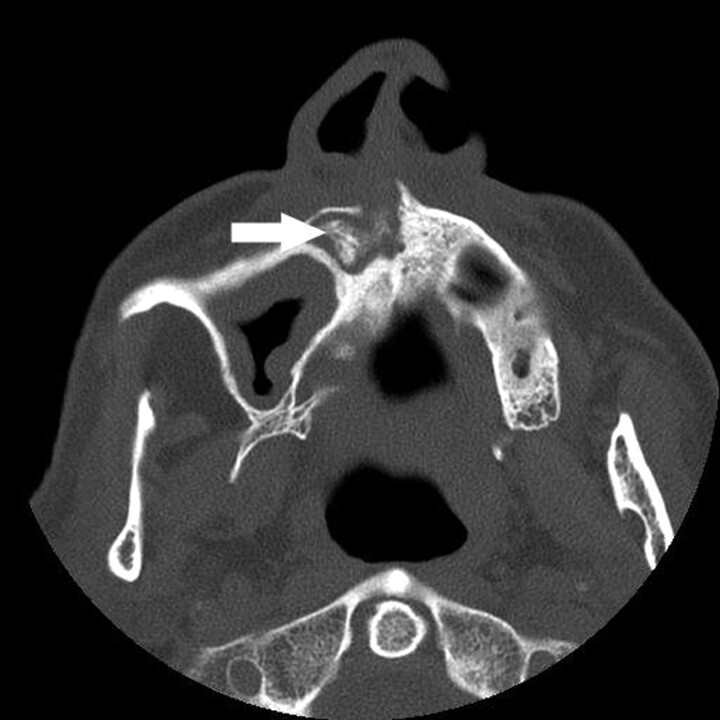
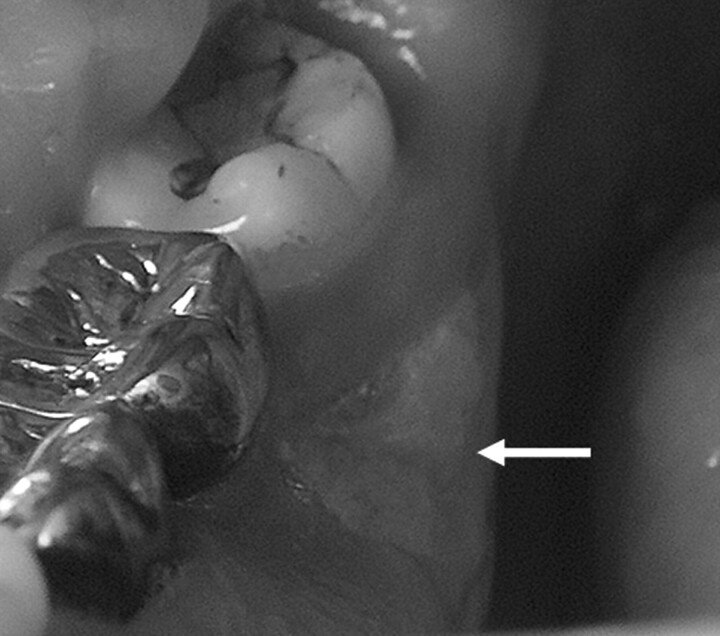
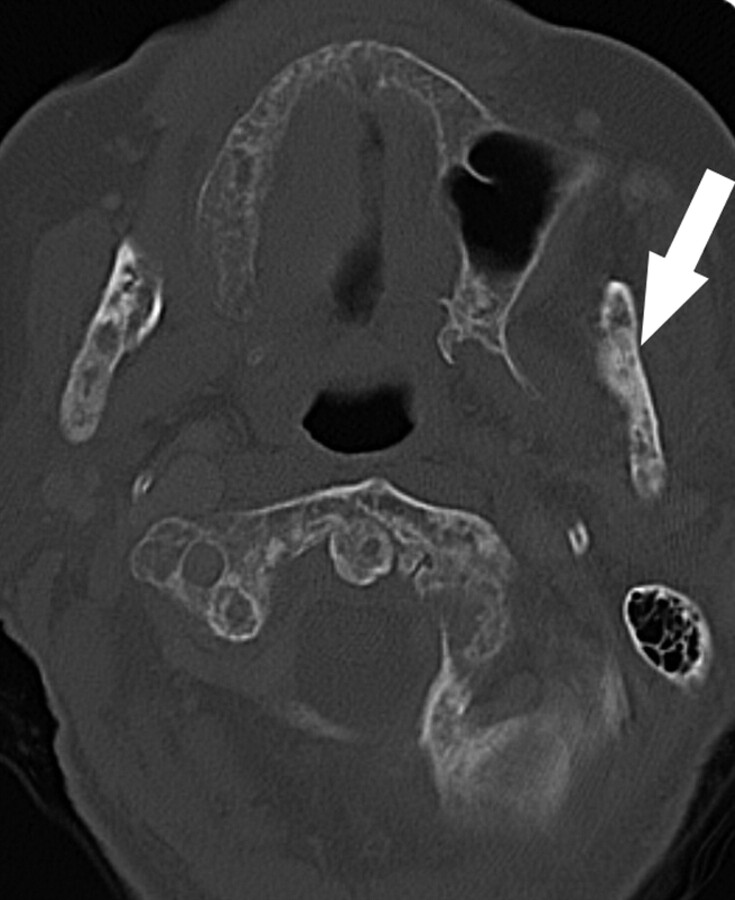
Results: All of the patients had a degree of osseous sclerosis, most commonly involving the alveolar margin, but lamina dura thickening and full-thickness sclerosis were also observed. The sclerotic change encroached on the mandibular canal in 3 patients. Less commonly encountered findings included poorly healing or nonhealing extraction sockets, periapical lucencies, widening of the periodontal ligament space, osteolysis, sequestra, oroantral fistula, soft tissue thickening, and periosteal new bone formation.
Conclusions: The most common finding in bisphosphonate-associated osteonecrosis was osseous sclerosis. This varied from subtle thickening of the lamina dura and alveolar crest to attenuated osteopetrosis-like sclerosis.
Figures



References
-
- Sparidans RW, Twiss IM, Talbot S. Bisphosphonates in bone diseases. Pharm World Sci 1998;20:206–13 - PubMed
-
- Marx RE. Pamidronate (Aredia) and zoledronate (Zometa) induced avascular necrosis of the jaws: a growing epidemic. J Oral Maxillofac Surg 2003;61:1115–17 - PubMed
-
- Ruggiero SL, Mehrotra B, Rosenberg TJ, et al. Osteonecrosis of the jaws associated with the use of bisphosphonates: a review of 63 cases. J Oral Maxillofac Surg 2004;62:527–34 - PubMed
-
- Marx RE, Sawatari Y, Fortin M, et al. Bisphosphonate-induced exposed bone (osteonecrosis/osteopetrosis) of the jaws: risk factors, recognition, prevention, and treatment. J Oral Maxillofac Surg 2005;63:1567–75 - PubMed
-
- Migliorati CA, Schubert MM, Peterson DE, et al. Bisphosphonate-associated osteonecrosis of mandibular and maxillary bone: an emerging oral complication of supportive cancer therapy. Cancer 2005;104:83–93 - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical