

Morphologic evaluation of the caudal end of the inferior petrosal sinus using 3D rotational venography
- PMID: 17569984
- PMCID: PMC8134147
- DOI: 10.3174/ajnr.A0489
Morphologic evaluation of the caudal end of the inferior petrosal sinus using 3D rotational venography
Abstract
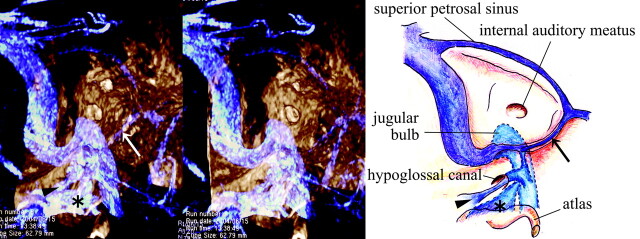
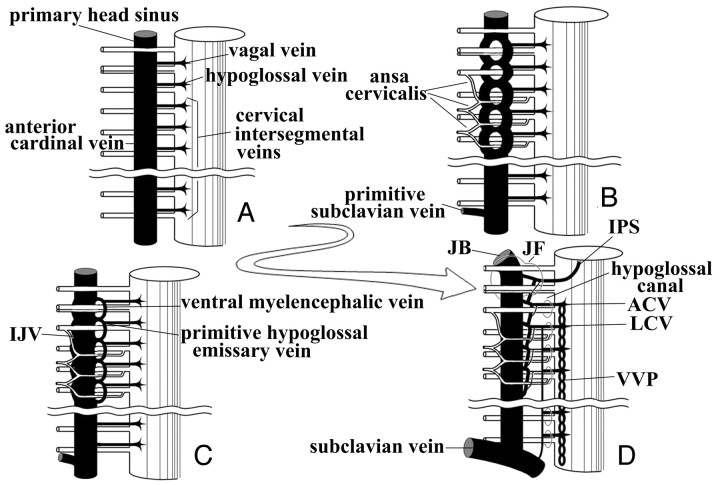
Background and purpose: The inferior petrosal sinus (IPS) is the main transvenous access route used to examine or treat lesions involving the cavernous sinus. To carry out these procedures successfully, one must have a detailed knowledge of the anatomy of the venous system around the junction of the IPS and the internal jugular vein (IJV).
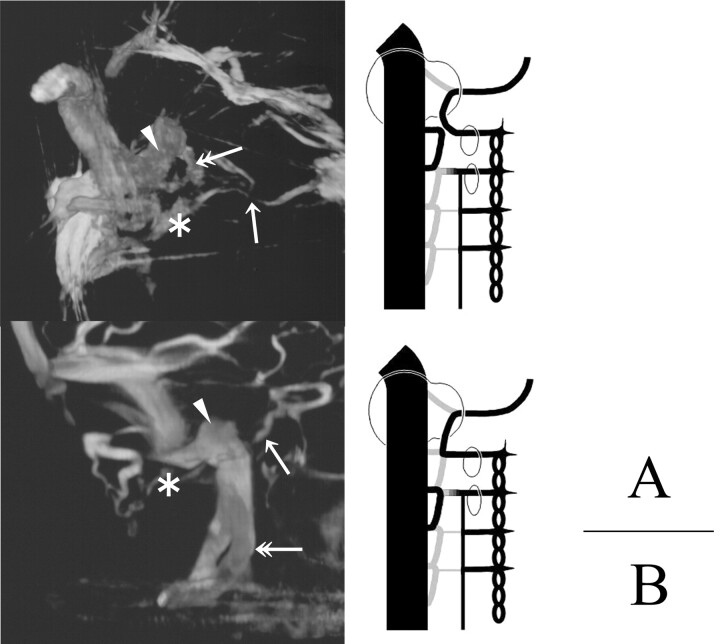
Materials and methods: Eighty-three sides in 63 patients (26 men, 37 women; mean, 56.5 years of age) were examined by using 3D rotational venography (3DRV).
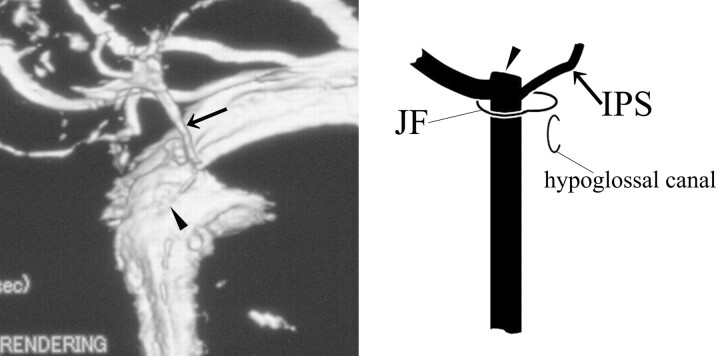
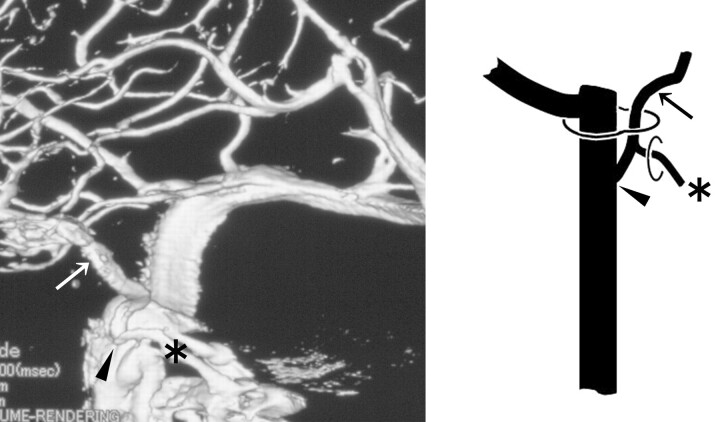
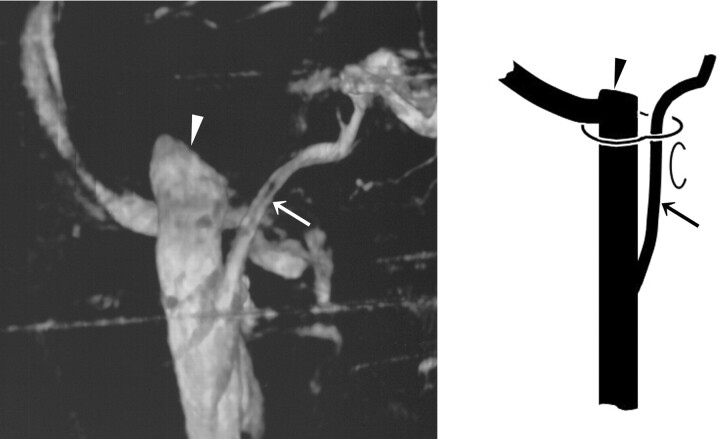
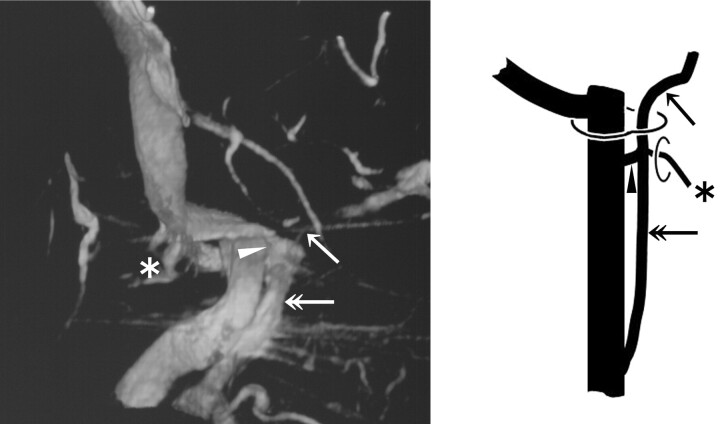
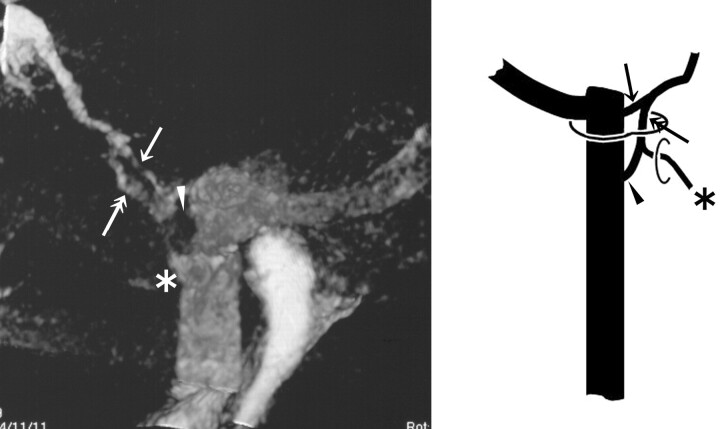
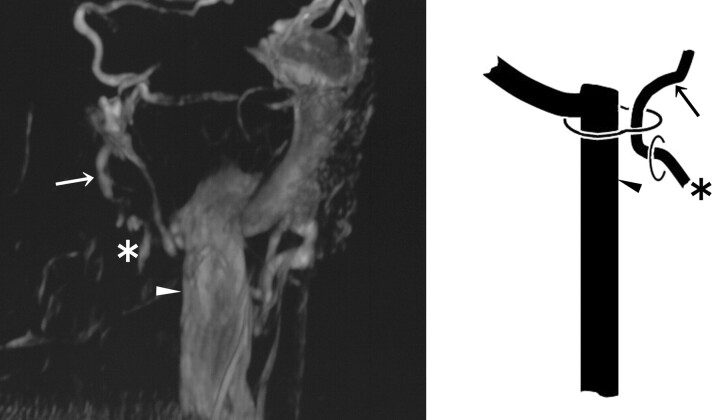
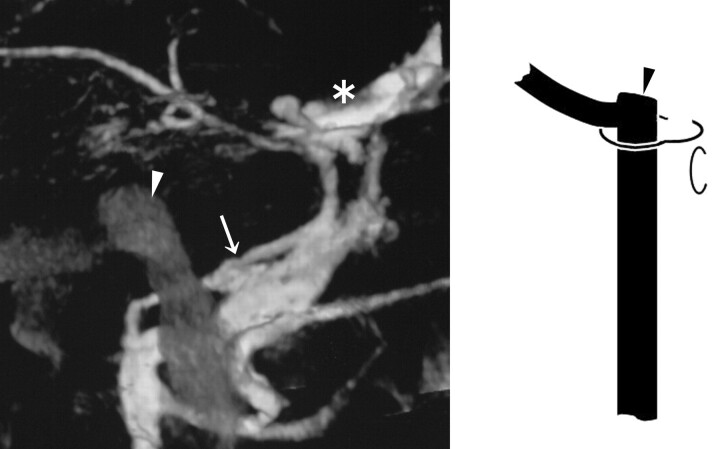
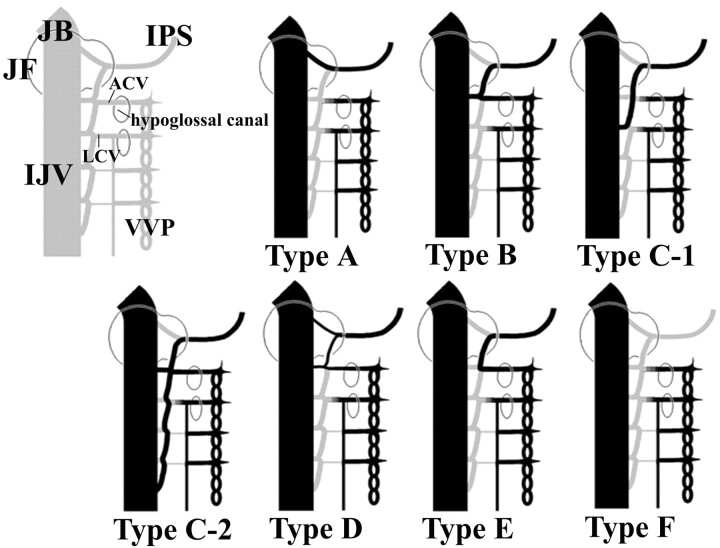
Result: The drainage patterns of the IPS could be classified into the following 6 types, with emphasis on the level of IPS-IJV junction: type A, the IPS drains into the jugular bulb in 1/83 sides (1.2%); type B, the IPS drains into the IJV at the level of the extracranial opening of the hypoglossal canal in 29/83 sides (34.9%); type C, the IPS drains into the lower extracranial IJV in 31/83 sides (37.3%); type D, the IPS forms a plexus and has multiple junctions to the IJV near the jugular foramen in 5/83 sides (6.0%); type E, the IPS drains directly into the vertebral venous plexus (VVP) with no connection to the IJV in 3/83 sides (3.6%); and type F, the IPS is absent in 14/83 sides (16.9%). Each type is also characterized by the way of anastomosis with the VVP.
Conclusion: This classification seemed to be rational from the embryologic viewpoint, and it may be useful in establishing treatment strategies that involve endovascular manipulation via the IPS.
Figures
References
-
- Katsuta T, Rhoton AL Jr, Matsushima T. The jugular foramen: microsurgical anatomy and operative approaches. Neurosurgery 1997;41:149–202 - PubMed
-
- Ayeni SA, Ohata K, Tanaka K, et al. The microsurgical anatomy of the jugular foramen. J Neurosurg 1995;83:903–09 - PubMed
-
- Shiu PC, Hanafee WN, Wilson GH, et al. Cavernous sinus venography. Am J Roentgenol Radium Ther Nucl Med 1968;104:57–62 - PubMed
-
- Miller DL, Doppmann JL. Petrosal sinus sampling: technique and rationale (comments). Radiology 1991;178:37–47 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources