

Use of dynamic microsimulation to predict disease progression in patients with pneumonia-related sepsis
- PMID: 17570835
- PMCID: PMC2206430
- DOI: 10.1186/cc5942
Use of dynamic microsimulation to predict disease progression in patients with pneumonia-related sepsis
Abstract
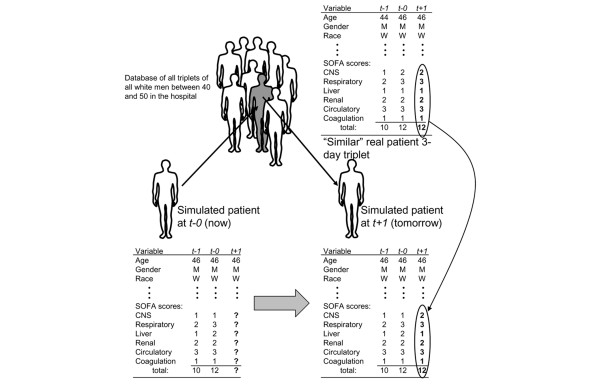
Introduction: Sepsis is the leading cause of death in critically ill patients and often affects individuals with community-acquired pneumonia. To overcome the limitations of earlier mathematical models used to describe sepsis and predict outcomes, we designed an empirically based Monte Carlo model that simulates the progression of sepsis in hospitalized patients over a 30-day period.
Methods: The model simulates changing health over time, as represented by the Sepsis-related Organ Failure Assessment (SOFA) score, as a function of a patient's previous health state and length of hospital stay. We used data from patients enrolled in the GenIMS (Genetic and Inflammatory Markers of Sepsis) study to calibrate the model, and tested the model's ability to predict deaths, discharges, and daily SOFA scores over time using different algorithms to estimate the natural history of sepsis. We evaluated the stability of the methods using bootstrap sampling techniques.
Results: Of the 1,888 patients originally enrolled, most were elderly (mean age 67.77 years) and white (80.72%). About half (47.98%) were female. Most were relatively ill, with a mean Acute Physiology and Chronic Health Evaluation III score of 56 and Pneumonia Severity Index score of 73.5. The model's estimates of the daily pattern of deaths, discharges, and SOFA scores over time were not statistically different from the actual pattern when information about how long patients had been ill was included in the model (P = 0.91 to 0.98 for discharges; P = 0.26 to 0.68 for deaths). However, model estimates of these patterns were different from the actual pattern when the model did not include data on the duration of illness (P < 0.001 for discharges; P = 0.001 to 0.040 for deaths). Model results were stable to bootstrap validation.
Conclusion: An empiric simulation model of sepsis can predict complex longitudinal patterns in the progression of sepsis, most accurately by models that contain data representing both organ-system levels of and duration of illness. This work supports the incorporation into mathematical models of disease of the clinical intuition that the history of disease in an individual matters, and represents an advance over several prior simulation models that assume a constant rate of disease progression.
Figures




Comment in
-
Between prediction, education, and quality control: simulation models in critical care.Crit Care. 2007;11(4):146. doi: 10.1186/cc5950. Crit Care. 2007. PMID: 17627804 Free PMC article.
References
-
- Anderson RN. Deaths: leading causes for 2000. Natl Vital Stat Rep. 2002;50:1–86. - PubMed
-
- Rangel-Frausto MS, Pittet D, Hwang T, Woolson RF, Wenzel RP. The dynamics of disease progression in sepsis: Markov modeling describing the natural history and the likely impact of effective antisepsis agents. Clin Infect Dis. 1998;27:185–190. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
