

Review
doi: 10.1007/s00247-007-0495-0.
Epub 2007 May 22.
Congenital anomalies of the male urethra
Affiliations
- PMID: 17572890
- PMCID: PMC1950215
- DOI: 10.1007/s00247-007-0495-0
Item in Clipboard
Review
Congenital anomalies of the male urethra
Pediatr Radiol.
2007 Sep.
Abstract
The spectrum of congenital anomalies of the male urethra is presented. The embryologic basis of each anomaly, when known, is discussed. Clinical and imaging features of each entity are presented.
Figures
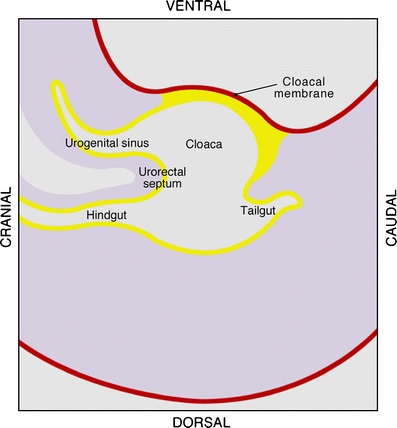
Embryologic development of the male genitourinary tract. The cloaca is divided into the urogenital sinus (precursor of the bladder and posterior urethra) and the hindgut by the urorectal septum (adapted from reference 2)
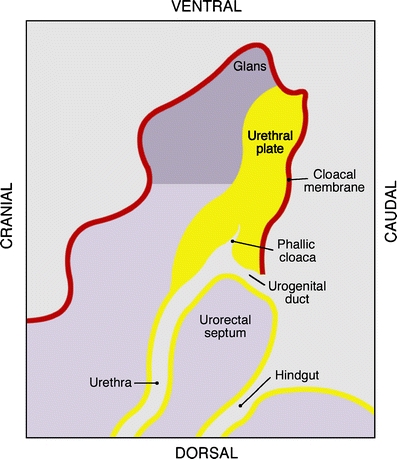
Embryologic development of the male genitourinary tract. The urorectal septum continues to descend and the cloacal membrane undergoes disruption. The hindgut and phallic cloaca now open separately to the exterior (adapted from reference 4)

Embryologic development of the male genitourinary tract. The phallic cloaca extends distally through the developing genital tubercle. Proliferation of rostral mesoderm of the genital tubercle displaces the cloaca so that it lies on the caudal aspect of the developing glans (adapted from reference 2)
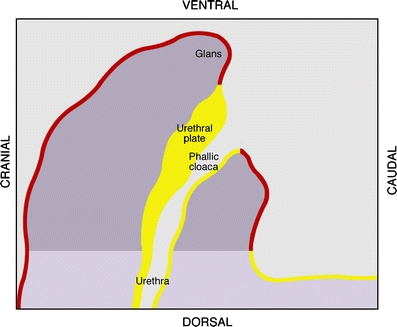
Embryologic development of the male genitourinary tract. Median cleavage of the urethral plate occurs. The urethral plate forms the deep and lateral walls of the proximal urethra. The phallic cloaca opens to the exterior at the base of the glans (adapted from reference 4)
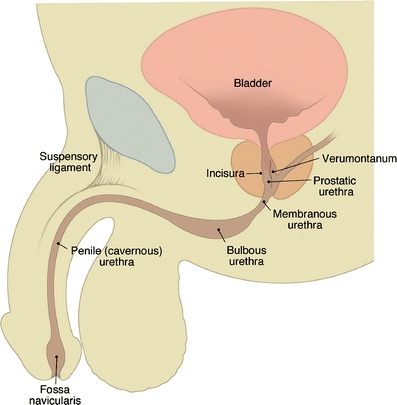
Normal male urethral anatomy
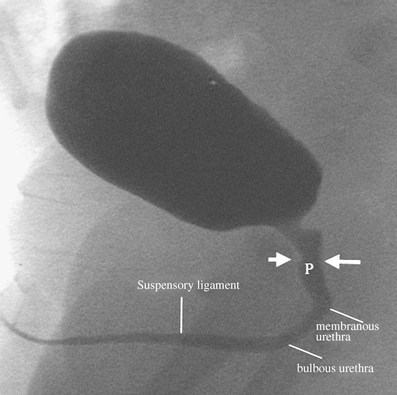
Voiding cystogram in a 3-year-old with prior urinary tract infection. Normal urethral anatomy is shown (P prostatic urethra, short arrow incisura, long arrow verumontanum)

Posterior urethral valves. Sonography demonstrates a thick-walled bladder and dilatation of the prostatic urethra (arrow), the “keyhole sign”
Posterior urethral valves. An image from a VCUG demonstrates a thick-walled trabeculated bladder and dilatation of the posterior urethra (long arrow), and the location of the valve (small arrow)
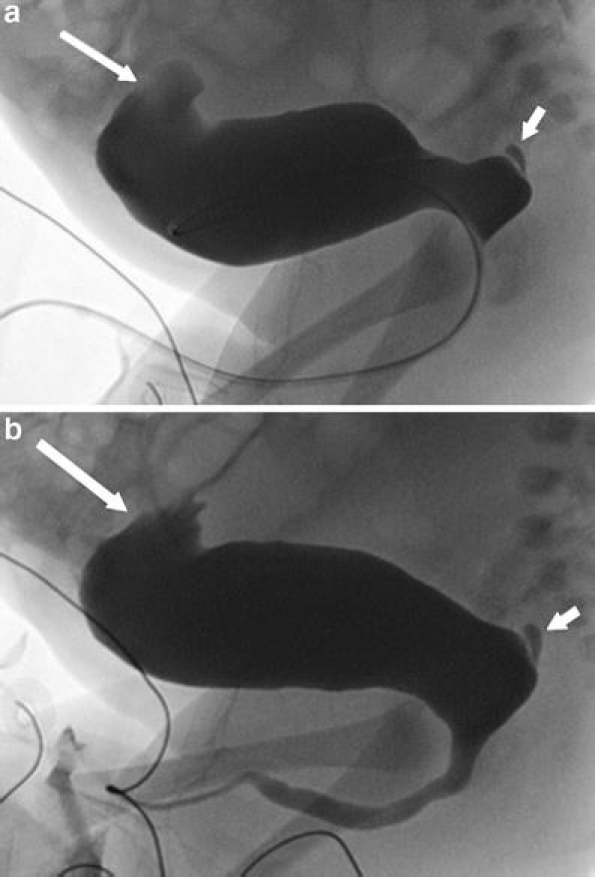
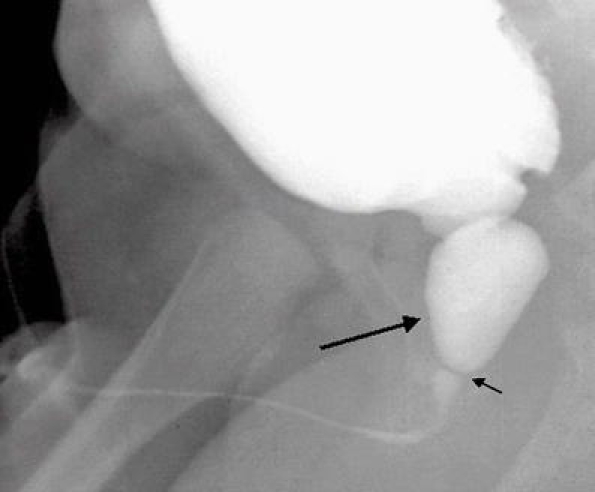
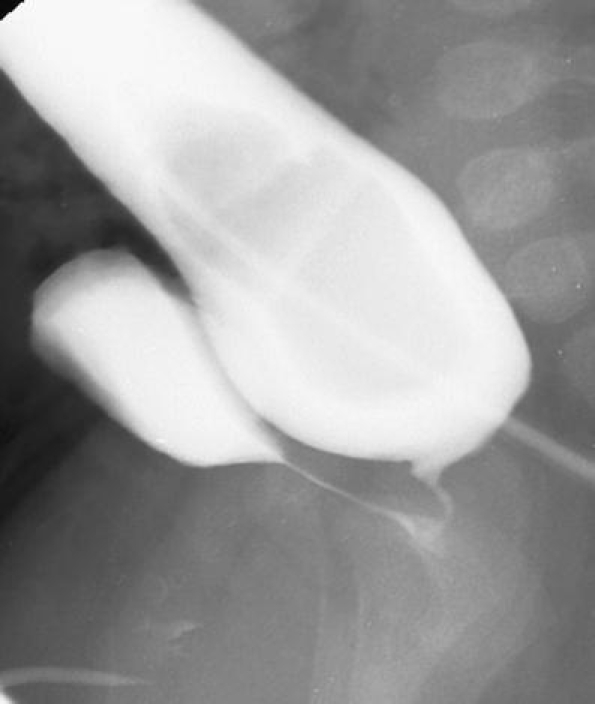
Prune-belly syndrome. a Images from a VCUG show the characteristic smooth-walled bladder that is tethered anteriorly by a urachal remnant (long arrow). Note the utricle (short arrow) arising from the dilated prostatic urethra, which is positioned dorsal to the wide bladder neck. b Voiding film shows dilatation of the proximal urethra consistent with megalourethra. Megalourethra can coexist in these patients

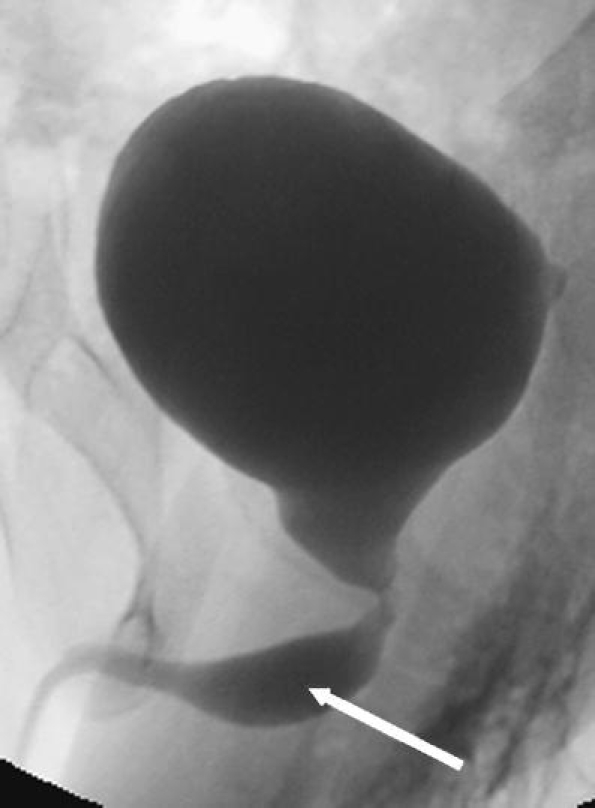
Congenital urethral stricture. A markedly dilated urethra is seen proximal to a congenital stricture in the bulbous urethra. Retrograde urethrography in this patient (not shown) demonstrated a focal narrowing at the bulbous urethra with a normal penile urethra. The site of obstruction is more distal than that seen with PUV
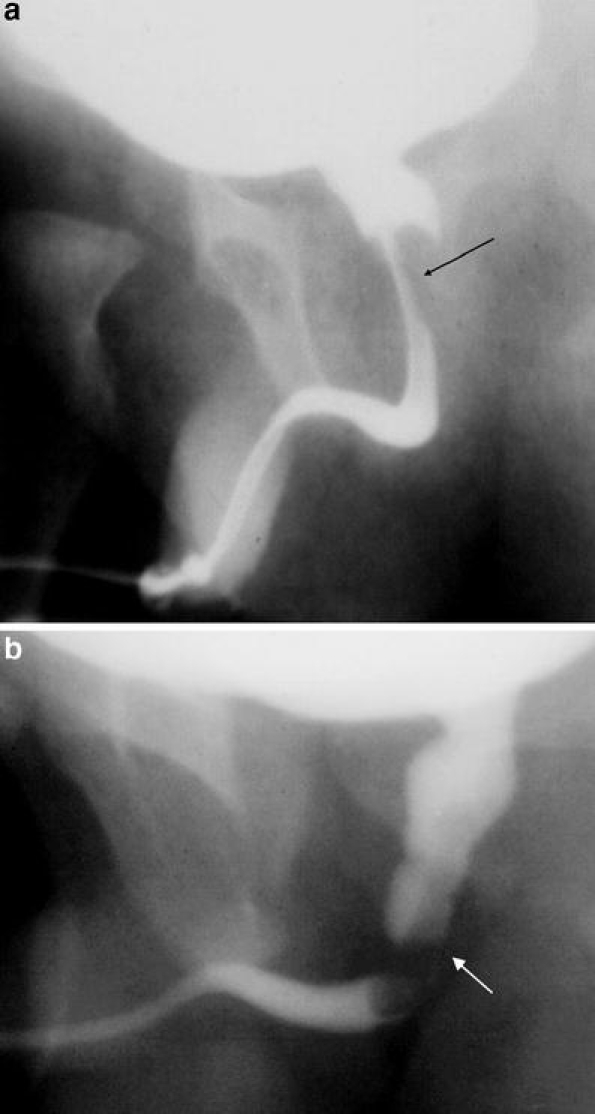
Urethral polyp. a Image from a VCUG demonstrates a polypoid filling defect arising from the prostatic urethra (arrow). b Note change of position of the filling defect (arrow) during the examination (images courtesy of J. Michael Zerin, MD)
Utricle. Voiding cystourethrogram in a child with urinary tract infection demonstrates a normal utricle that was incidentally detected (arrow). The ventral urethra is not filled with contrast material
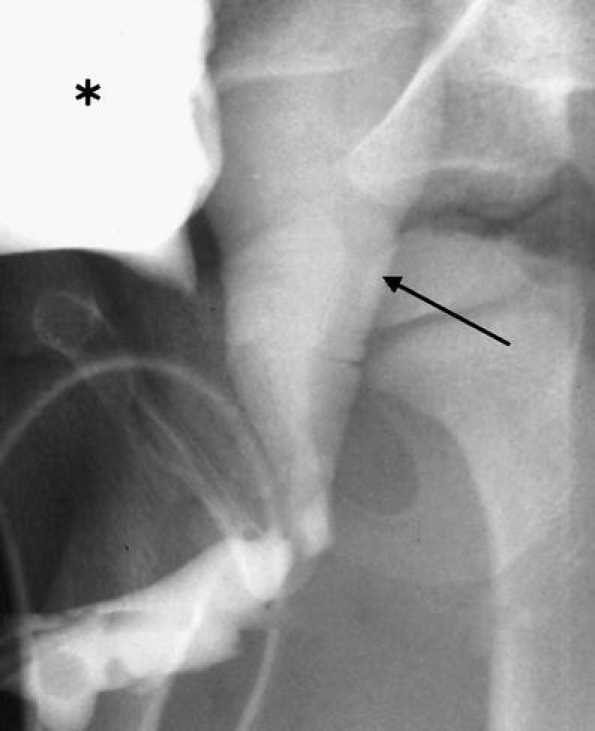
Enlarged prostatic utricle. There is filling of a large utricle (arrow) that arises from and communicates with the posterior urethra in this patient with intersex abnormality. The patient has had penile urethral reconstruction (asterisk bladder)
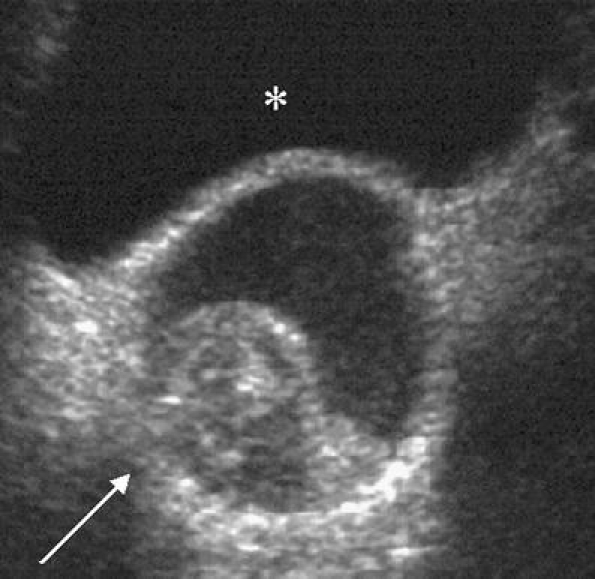
Mullerian duct cyst. Transverse sonographic image of the bladder in this 15-year-old boy with recurrent epididymitis demonstrates a cystic mass with internal debris (arrow) posterior to the bladder (asterisk)
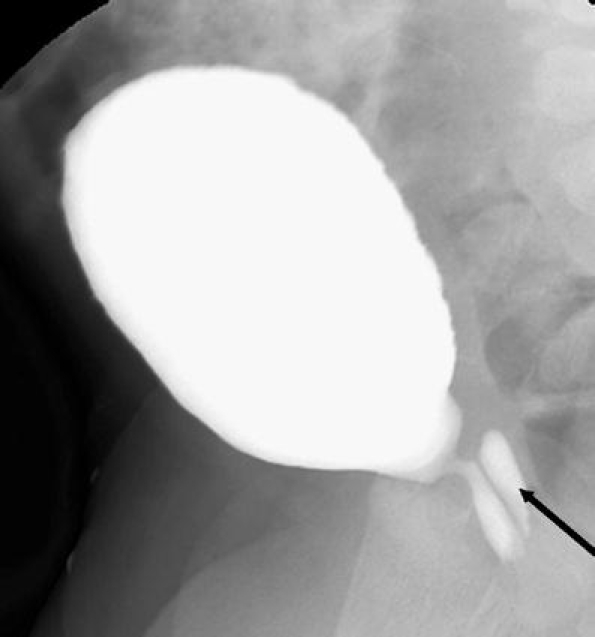
Cowper’s gland. During voiding there is filling of a structure at the ventral aspect of the bulbourethra (arrow)

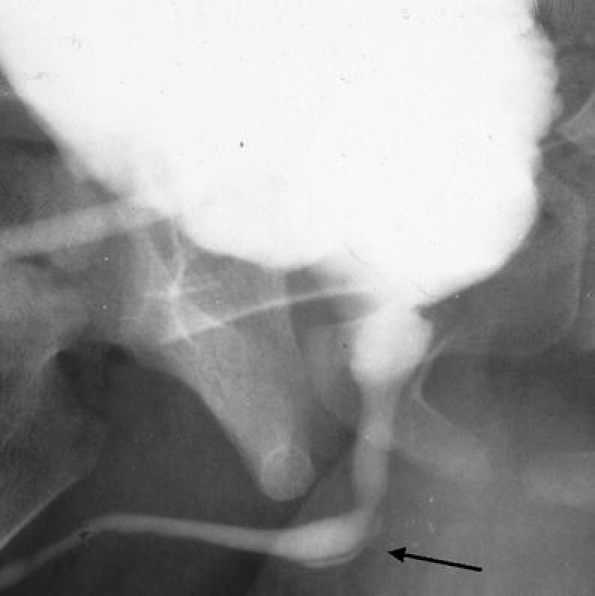
Anterior urethral diverticulum. Arrow points to a diverticulum arising from and communicating with the ventral aspect of the urethra

Valves of Guerin. A small contrast-filled diverticulum (arrow) is present, arising from the dorsal aspect of the glans urethra. There is no urethral obstruction
Megalourethra. Single view from a VCUG in a boy with partial sacral agenesis demonstrates focal dilatation of the urethra (arrow). Note the wide bladder neck

Complete urethral duplication (type II). Image from a voiding cystourethrogram demonstrates contrast agent filling a dorsal and ventral urethra (arrows). Vesicoureteral reflux is present
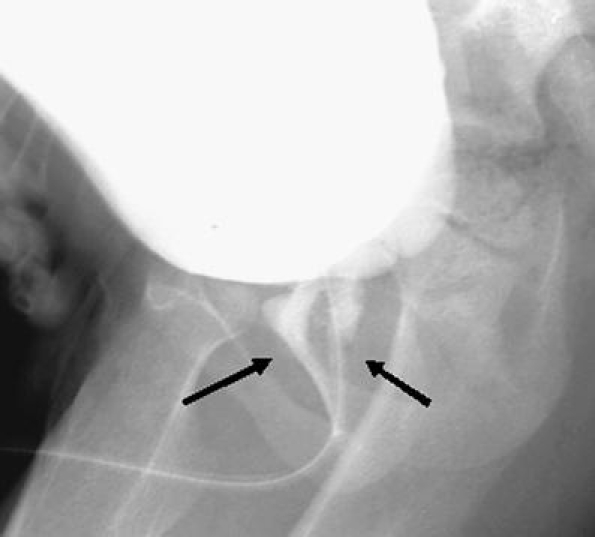
Partial urethral duplication (type I). There is partial duplication of the urethra in this patient with a history of hypospadias repair. The two channels (arrows) join to a single channel, which is demarcated by the catheter

Anorectal malformation. Image from a VCUG demonstrates an anourethral fistula (arrow) in a newborn. This is also referred to as an H-type fistula because of its configuration
Anorectal malformation. Distal loop study in an infant with a high imperforate anus demonstrates a fistula extending from the rectum to the posterior urethra
References
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.1016/S0022-5347(05)00642-7', 'is_inner': False, 'url': 'https://doi.org/10.1016/s0022-5347(05)00642-7'}, {'type': 'PubMed', 'value': '16515962', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/16515962/'}]}
- Krishan A, de Souza A, Konijeti R et al (2006) The anatomy and embryology of posterior urethral valves. J Urol 175:1214–1220 - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.1016/j.bjps.2003.08.019', 'is_inner': False, 'url': 'https://doi.org/10.1016/j.bjps.2003.08.019'}, {'type': 'PubMed', 'value': '14672675', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/14672675/'}]}
- Hynes PJ, Fraher JP (2004) The development of the male genitourinary system I: the origin of the urorectal septum and the formation of the perineum. Br J Plast Surg 57:27–36 - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.1016/j.bjps.2003.08.018', 'is_inner': False, 'url': 'https://doi.org/10.1016/j.bjps.2003.08.018'}, {'type': 'PubMed', 'value': '15037165', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/15037165/'}]}
- Hynes PJ, Fraher JP (2004) The development of the male genitourinary system II: the origin and formation of the urethral plate. Br J Plast Surg 57:112–121 - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.1016/j.bjps.2003.08.017', 'is_inner': False, 'url': 'https://doi.org/10.1016/j.bjps.2003.08.017'}, {'type': 'PubMed', 'value': '15006521', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/15006521/'}]}
- Hynes PJ, Fraher JP (2004) The development of the male genitourinary system III: the formation of the spongiose and glandar urethra. Br J Plast Surg 57:203–214 - PubMed
-
- None
- Gray H (1973) The urogenital system. In: Goss CM (ed) Gray’s anatomy of the human body. Lea and Febiger, Philadelphia, pp 1296–1297
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
