

Risk factors for 30-day mortality after resection of lung cancer and prediction of their magnitude
- PMID: 17573442
- PMCID: PMC2117132
- DOI: 10.1136/thx.2007.079145
Risk factors for 30-day mortality after resection of lung cancer and prediction of their magnitude
Abstract
Background: There is considerable variability in reported postoperative mortality and risk factors for mortality after surgery for lung cancer. Population-based data provide unbiased estimates and may aid in treatment selection.
Methods: All patients diagnosed with lung cancer in Norway from 1993 to the end of 2005 were reported to the Cancer Registry of Norway (n = 26 665). A total of 4395 patients underwent surgical resection and were included in the analysis. Data on demographics, tumour characteristics and treatment were registered. A subset of 1844 patients was scored according to the Charlson co-morbidity index. Potential factors influencing 30-day mortality were analysed by logistic regression.
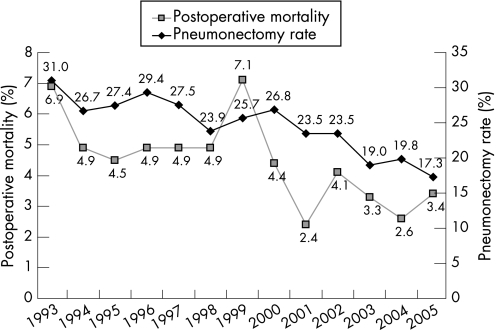
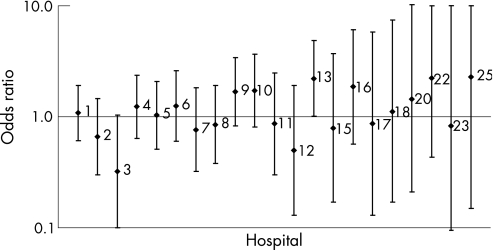
Results: The overall postoperative mortality rate was 4.4% within 30 days with a declining trend in the period. Male sex (OR 1.76), older age (OR 3.38 for age band 70-79 years), right-sided tumours (OR 1.73) and extensive procedures (OR 4.54 for pneumonectomy) were identified as risk factors for postoperative mortality in multivariate analysis. Postoperative mortality at high-volume hospitals (> or = 20 procedures/year) was lower (OR 0.76, p = 0.076). Adjusted ORs for postoperative mortality at individual hospitals ranged from 0.32 to 2.28. The Charlson co-morbidity index was identified as an independent risk factor for postoperative mortality (p = 0.017). A prediction model for postoperative mortality is presented.
Conclusions: Even though improvements in postoperative mortality have been observed in recent years, these findings indicate a further potential to optimise the surgical treatment of lung cancer. Hospital treatment results varied but a significant volume effect was not observed. Prognostic models may identify patients requiring intensive postoperative care.
Conflict of interest statement
Competing interests: None.
Comment in
-
Risk and benefit: the eternal Yin and Yang of thoracic surgery.Thorax. 2007 Nov;62(11):929-30. doi: 10.1136/thx.2007.082982. Thorax. 2007. PMID: 17965075 Free PMC article.
References
-
- Cancer Registry of Norway Cancer in Norway 2005. 2006. http://www.kreftregisteret.no/forekomst_og_overlevelse_2005/cin2005.pdf
MeSH terms
LinkOut - more resources
Full Text Sources
Medical