

Review
doi: 10.1161/HYPERTENSIONAHA.107.091322.
Epub 2007 Jun 18.
Potential roles of angiotensin receptor-activating autoantibody in the pathophysiology of preeclampsia
Affiliations
- PMID: 17576854
- PMCID: PMC3261616
- DOI: 10.1161/HYPERTENSIONAHA.107.091322
Item in Clipboard
Review
Potential roles of angiotensin receptor-activating autoantibody in the pathophysiology of preeclampsia
Hypertension.
2007 Aug.
No abstract available
Figures
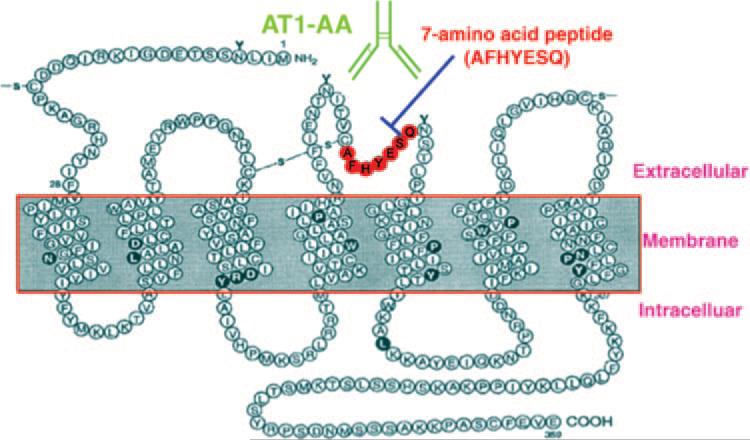
Schematic diagrams of AT1 receptor and the sequence of 7 amino acid antibody blocking epitope peptide. AT1-AA interacts with second extracellular loop of AT1 receptor. This interaction can be blocked by a specific 7 amino acid peptide.
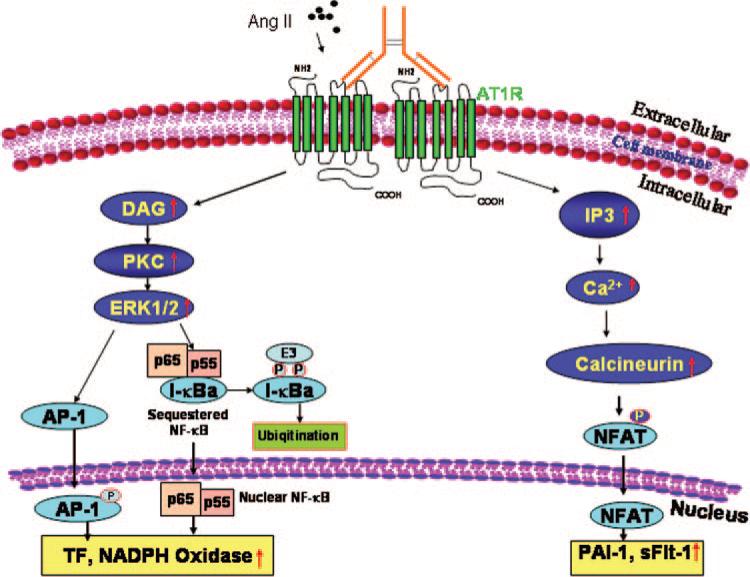
Molecular mechanism of AT1-AA–mediated AT1 receptor activation. Multiple signaling pathways function downstream of AT1-AA–mediated AT1 receptor activation. AT1-AA–mediated AT1 receptor activation leads to increased PKC and calcineurin activity. As a result, downstream transcription factors, such as activating protein-1, nuclear factor κB (NF-κB), and nuclear factor activating T cell (NFAT), are activated and translocate from cytosol to nucleus, leading to increased gene expression. Because AT1 activating autoanti-bodies are bivalent IgG protein complexes, we propose that they exert their agonistic effect by cross-linking and thereby stabilizing AT1 receptor homodimers. DAG indicates diacylglycerol; IP3, inositol triphosphate; PKC, protein kinase C.
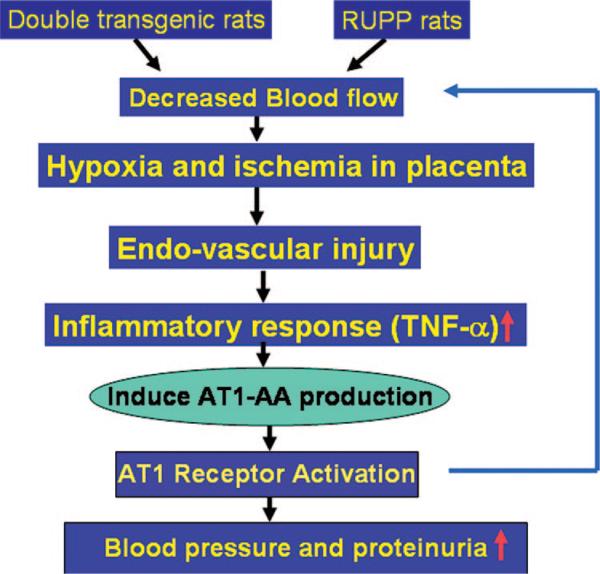
Molecular basis of AT1-AA production in rat models of preeclampsia: generation of AT1-AA may be secondary to placental ischemia, vascular damage, and enhanced inflammatory response. The decreased blood flow to placenta in double transgenic rats and RUPP rats leads to placental ischemia and hypoxia. This will result in endovascular damage and the enhanced inflammatory response with increased secretion of inflammatory cytokines (eg, TNF-α). The resulting inflammatory cytokine secretion contributes to AT1 receptor agonistic antibody production. AT1-AA will directly induce higher blood pressure and proteinuria via AT1 receptor activation. This may eventually lead more hypoxia, endovascular damage, and enhanced inflammatory response. Thus, we speculate that hypoxia because of reduced placental perfusion may lead to an inflammatory response that contributes to the generation of AT1-AA. The resulting AT1-AA may further contribute to decreased trophoblast invasion, increased hypoxia, and an enhanced inflammatory response, leading to more AT1-AA production. Therefore, reduced placental perfusion, hypoxia, inflammatory response, and AT1-AA production act as a detrimental cycle to contribute to pathophysiology of preeclampsia.
References
-
- Walker JJ. Pre-eclampsia. Lancet. 2000;356:1260–1265. - PubMed
-
- Roberts JM. Endothelial dysfunction in preeclampsia. Semin Reprod Endocrinol. 1998;16:5–15. - PubMed
-
- Roberts JM, Cooper DW. Pathogenesis and genetics of pre-eclampsia. Lancet. 2001;357:53–56. - PubMed
-
- Roberts JM, Lain KY. Recent insights into the pathogenesis of preeclampsia. Placenta. 2002;23:359–372. - PubMed
-
- Roberts JM, Edep ME, Goldfien A, Taylor RN. Sera from preeclamptic women specifically activate human umbilical vein endothelial cells in vitro: morphological and biochemical evidence. Am J Reprod Immunol. 1992;27:101–108. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
