

Anterior vaginal wall length and degree of anterior compartment prolapse seen on dynamic MRI
- PMID: 17579801
- PMCID: PMC2289388
- DOI: 10.1007/s00192-007-0405-x
Anterior vaginal wall length and degree of anterior compartment prolapse seen on dynamic MRI
Erratum in
- Int Urogynecol J Pelvic Floor Dysfunct. 2014 Oct;25(10):1447. DeLancey, James O L [corrected to DeLancey, John O L]
Abstract
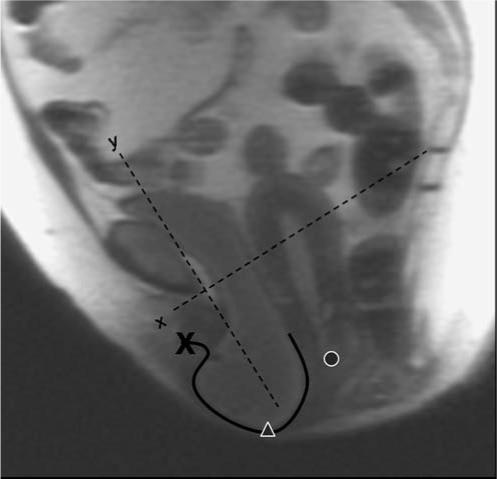
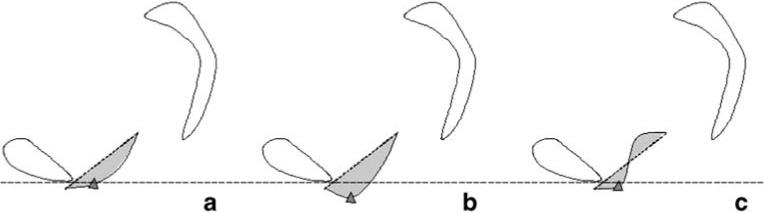
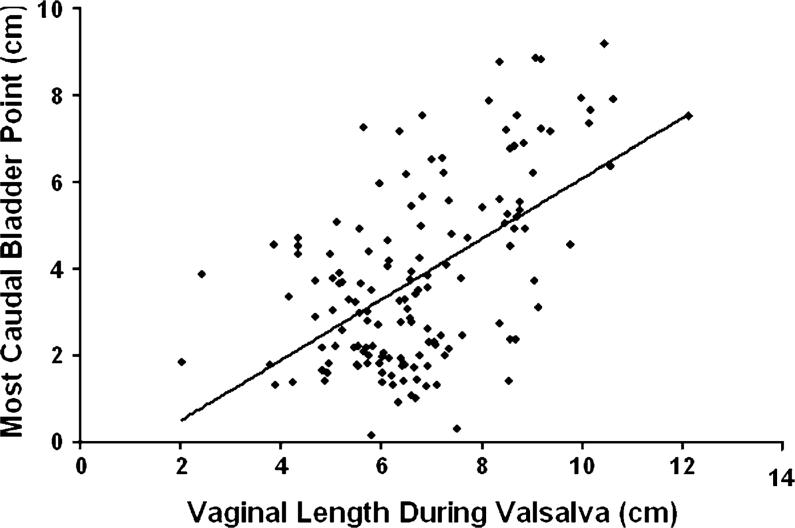
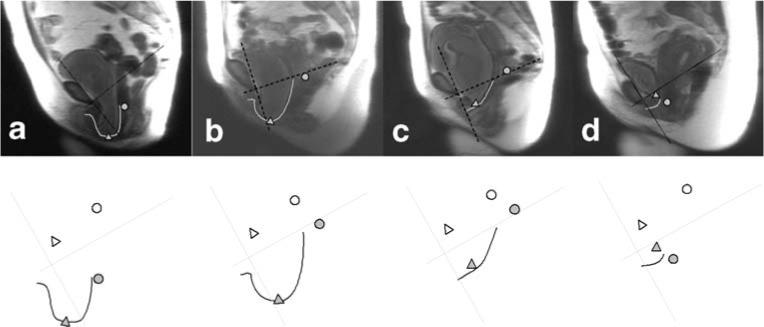
The objective of the study was to determine the relationship between midsagittal vaginal wall geometric parameters and the degree of anterior vaginal prolapse. We have previously presented data indicating that about half of anterior wall descent can be explained by the degree of apical descent present (Summers et al., Am J Obstet Gynecol, 194:1438-1443, 2006). This led us to examine whether other midsagittal vaginal geometric parameters are associated with anterior wall descent. Magnetic resonance (MR) scans of 145 women from the prior study were suitable for analysis after eight were excluded because of inadequate visibility of the anterior vaginal wall. Subjects had been selected from a study of pelvic organ prolapse that included women with and without prolapse. All patients underwent supine dynamic MR scans in the midsagittal plane. Anterior vaginal wall length, location of distal vaginal wall point, and the area under the midsagittal profile of the anterior vaginal wall were measured during maximal Valsalva. A linear regression model was used to examine how much of the variance in cystocele size could be explained by these vaginal parameters. When both apical descent and vaginal length were considered in the linear regression model, 77% (R (2) = 0.77, p < 0.001) of the variation in anterior wall descent was explained. Distal vaginal point and a measure anterior wall shape, the area under the profile of the anterior vaginal wall, added little to the model. Increasing vaginal length was positively correlated with greater degrees of anterior vaginal prolapse during maximal Valsalva (R (2) = 0.30, p < 0.01) determining 30% of the variation in anterior wall decent. Greater degrees of anterior vaginal prolapse are associated with a longer vaginal wall. Linear regression modeling suggests that 77% of anterior wall descent can be explained by apical descent and midsagittal anterior vaginal wall length.
Figures
References
-
- Hendrix SL, Clark A, Nygaard I, Aragaki A, Barnabei V, McTiernan A. Pelvic organ prolapse in the Women's Health Initiative: gravity and gravidity. Am J Obstet Gynecol. 2002;186(6):1160–1166. - PubMed
-
- Shull BL, Bachofen C, Coates KW, Kuehl TJ. A transvaginal approach to repair of apical and other associated sites of pelvic organ prolapse with uterosacral ligaments. Am J Obstet Gynecol. 2000;183:1365–1373. - PubMed
-
- Weber AM, Walters MD, Piedmonte MR, Ballard LA. Anterior colporrhaphy: a randomized trial of three surgical techniques. Am J Obstet Gynecol. 2001;185:1299–1304. - PubMed
-
- DeLancey JO, Morgan DM, Fenner DE, Kearney R, Guire K, Miller JM, Hussain H, Umek W, Hsu Y, Ashton-Miller JA. Comparison of levator ani muscle defects and function in women with and without pelvic organ prolapse. Obstet Gynecol. 2007;109:295–302. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical