

An economic evaluation of prolonged mechanical ventilation
- PMID: 17581479
- PMCID: PMC2745076
- DOI: 10.1097/01.CCM.0000275391.35834.10
An economic evaluation of prolonged mechanical ventilation
Abstract
Objective: Patients who receive prolonged mechanical ventilation have high resource utilization and relatively poor outcomes, especially the elderly, and are increasing in number. The economic implications of prolonged mechanical ventilation provision, however, are uncertain and would be helpful to providers and policymakers. Therefore, we aimed to determine the lifetime societal value of prolonged mechanical ventilation.
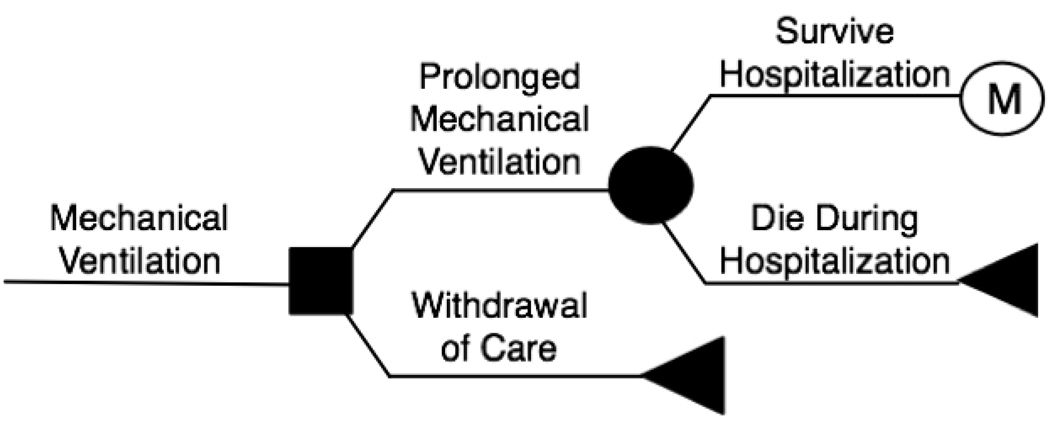
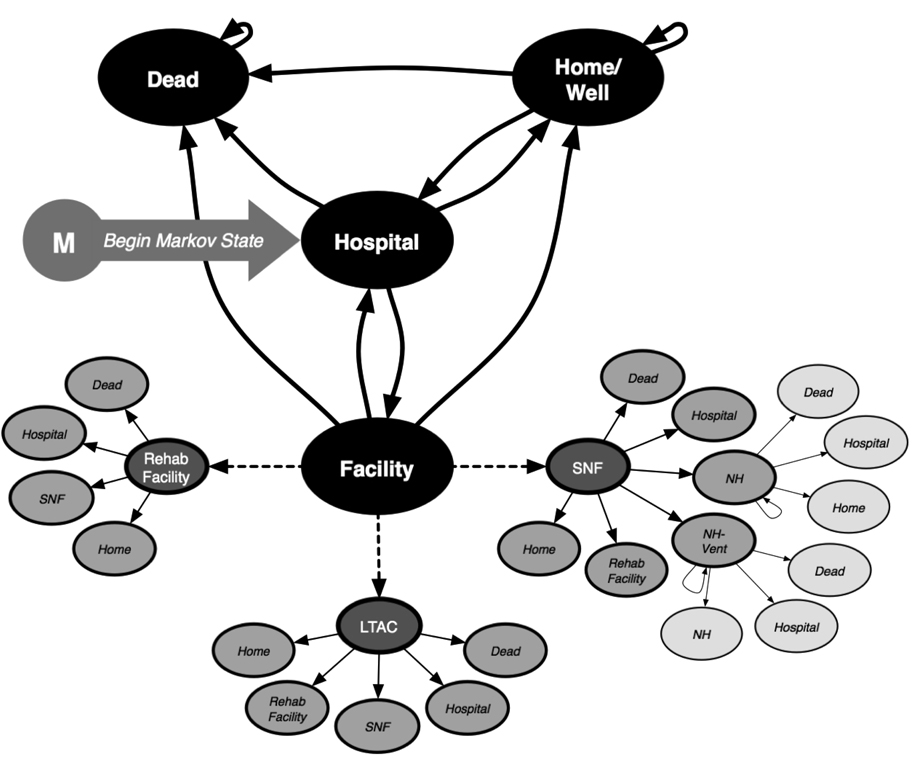
Design and patients: Adopting the perspective of a healthcare payor, we developed a Markov model to determine the cost effectiveness of providing mechanical ventilation for at least 21 days to a 65-yr-old critically ill base-case patient compared with the provision of comfort care resulting in withdrawal of ventilation. Input data were derived from the medical literature, Medicare, and a recent large cohort study of ventilated patients.
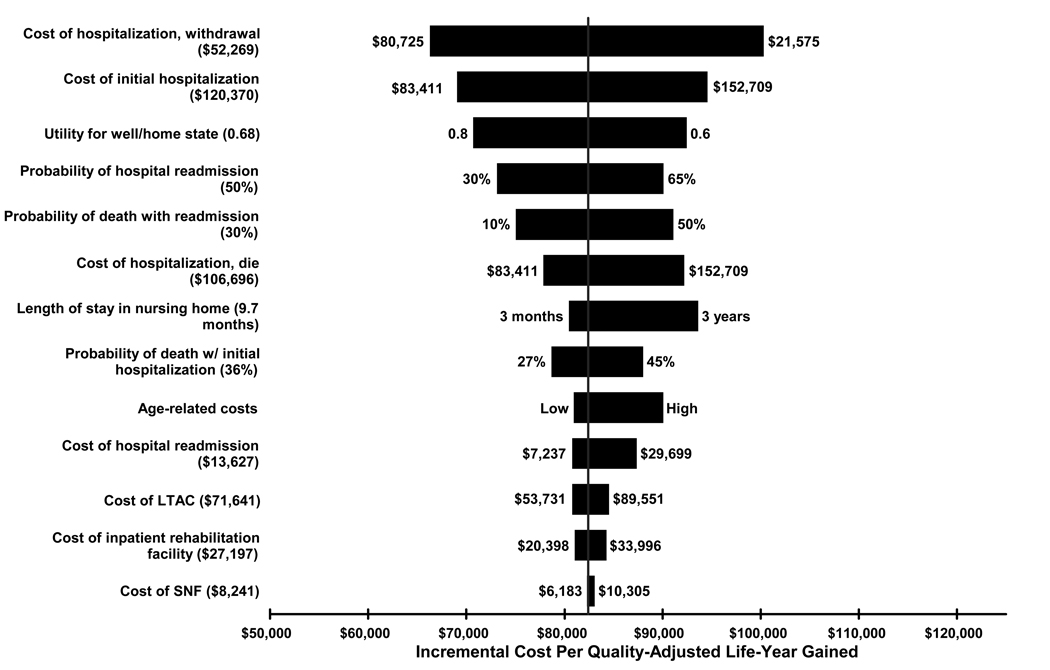
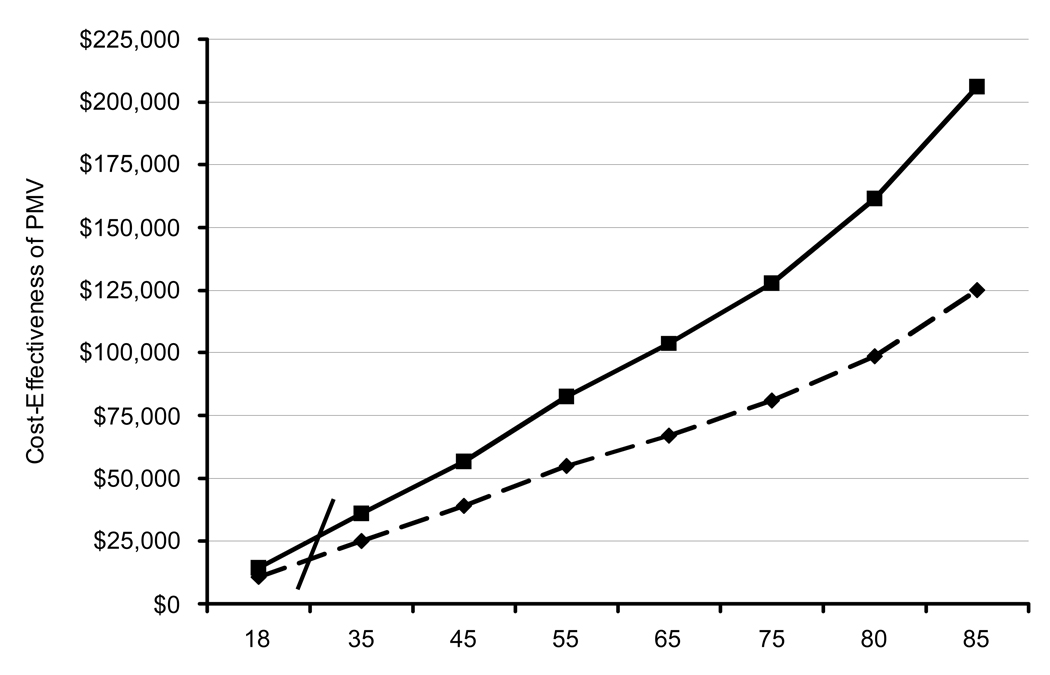
Measurements and main results: We determined lifetime costs and survival, quality-adjusted life expectancy, and cost effectiveness as reflected by costs per quality-adjusted life-year gained. Providing prolonged mechanical ventilation to the base-case patient cost "dollars"55,460 per life-year gained and "dollars"82,411 per quality-adjusted life-year gained compared with withdrawal of ventilation. Cost-effectiveness ratios were most sensitive to variation in age, hospital costs, and probability of readmission, although less sensitive to postacute care-facility costs. Specifically, incremental costs per quality-adjusted life-year gained by prolonged mechanical ventilation provision exceeded "dollars"100,000 with age >or=68 and when predicted 1-yr mortality was >50%.
Conclusions: The cost effectiveness of prolonged mechanical ventilation provision varies dramatically based on age and likelihood of poor short- and long-term outcomes. Identifying patients likely to have unfavorable outcomes, lowering intensity of care for appropriate patients, and reducing costly readmissions should be future priorities in improving the value of prolonged mechanical ventilation.
Figures
Comment in
-
The costs of prolonged mechanical ventilation: how much is too much?Crit Care Med. 2007 Aug;35(8):1994. doi: 10.1097/01.CCM.0000277517.43175.FC. Crit Care Med. 2007. PMID: 17667253 No abstract available.
-
Prolonged mechanical ventilation is even more expensive.Crit Care Med. 2007 Dec;35(12):2881; author reply 2881-2. doi: 10.1097/01.CCM.0000295467.41730.DB. Crit Care Med. 2007. PMID: 18043220 No abstract available.
References
-
- Kersten A, Millbrandt MB, Rahim MT, et al. How big is critical care in the US? Crit Care Med. 2004:A8.
-
- Carson SS, Bach PB. The epidemiology and costs of chronic critical illness. Crit Care Clin. 2002;18:461–476. - PubMed
-
- Seneff MG, Zimmerman JE, Knaus WA, et al. Predicting the duration of mechanical ventilation: the importance of disease and patient characteristics. Chest. 1996;110:469–479. - PubMed
-
- MacIntyre NR, Epstein SK, Carson S, et al. Management of patients requiring prolonged mechanical ventilation: report of a NAMDRC consensus conference. Chest. 2005;128:3937–3954. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
