

Clinical outcome of fractures of the talar body
- PMID: 17583811
- PMCID: PMC2898957
- DOI: 10.1007/s00264-007-0399-5
Clinical outcome of fractures of the talar body
Abstract
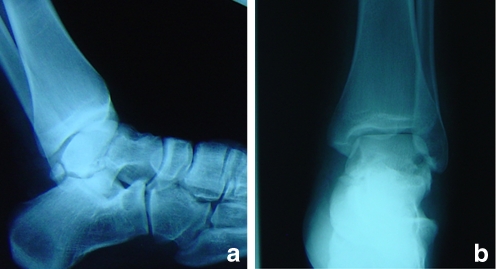
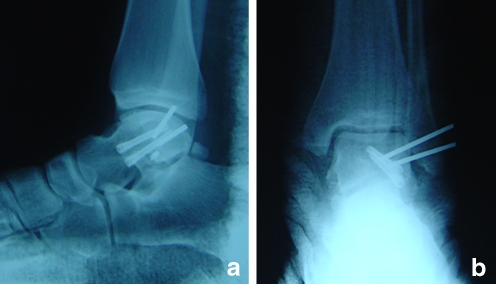
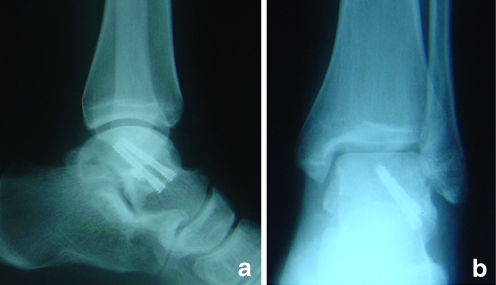
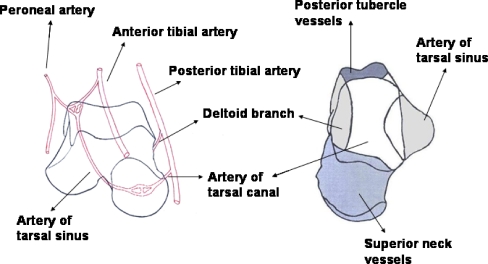
Fractures of the talar body present a great challenge to surgeons due to their rarity and high incidence of sequelae. This study reports the medium-term results of displaced fractures of the talar body treated by internal fixation. Nineteen patients (13 M, 6 F, mean age 31) with talar body fractures were studied retrospectively to assess outcome after operative treatment. The fractures were classified as coronal (11), sagittal (6) and crush fractures (2). Six patients sustained open fractures and two had associated talar neck fractures. Average follow-up was 26 months (range: 18-43). Clinical outcome based on American Orthopaedic Foot & Ankle Society (AOFAS) ankle-hindfoot scoring was excellent function in four patients, good in six, fair in four and poor in five. Early complications included two superficial wound infections, one partial wound dehiscence, one instance of skin necrosis and one deep infection. Other complications included delayed union in one, avascular necrosis in seven and malunion in one patient. Talar injuries are serious because they can compromise motion of the foot and ankle and result in severe disability. Crush fractures of the talar body and those associated with open injuries and talar neck fractures are associated with a less favourable outcome.
Les fractures du corps du talus sont difficiles à traiter pour les chirurgiens. Cette étude rapporte le traitement à moyen terme des fractures déplacées du talus par fixation interne. 19 patients (13 garçons, 6 filles d’un âge moyen de 31 ans). Les fractures ont été classées de la façon suivante : fractures coronales 11, fractures saggitales 6 et écrasement, fractures 2. Six patients présentaient une fracture ouverte et deux une fracture du col. Le suivi moyen a été de 26 mois (de 18 à 43 mois). L’évaluation clinique des patients a été réalisée selon le score de la Foot & Ankle Society (AOFAS). Le résultat au niveau de la cheville et de l’arrière pied est excellent sur le plan fonctionnel chez 4 patients, bon chez 6 patients, moyen chez 4 patients et mauvais chez 5 patients. Les complications précoces ont été les suivantes : deux infections superficielles, une nécrose cutanée, et une infection profonde. Les autres complications ont été les suivantes : retard de consolidation chez un patient, nécrose avasculaire chez sept patients et pseudarthrose chez un patient. Les traumatismes du talus sont des lésions relativement sérieuses et peuvent compromettre la mobilité du pied et de la cheville. Lorsqu’il y a association d’une fracture écrasement et de lésions cutanées. De telles fractures entraînent souvent un mauvais résultat fonctionnel.
Figures
References
-
- Alvarez RG. Talar neck fractures. In: Myerson M, editor. Current therapy in foot and ankle surgery. St. Louis: Mosby; 1993. pp. 243–248.
-
- Boyd HB, Knight RA. Fractures of the astragalus. South Med J. 1942;35:160–167.
-
- Coltart WD. Aviator’s astragalus. J Bone Joint Surg Br. 1952;34:545–566. - PubMed
-
- Elgafy H, Ebraheim NA, Tile M, Stephen D, Kase J. Fractures of the talus: experience of two level 1 trauma centers. Foot Ankle Int. 2000;21:1023–1029. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
