

Hyperplastic polyposis associated with two asynchronous colon cancers
- PMID: 17589908
- PMCID: PMC4436615
- DOI: 10.3748/wjg.v13.i23.3255
Hyperplastic polyposis associated with two asynchronous colon cancers
Abstract
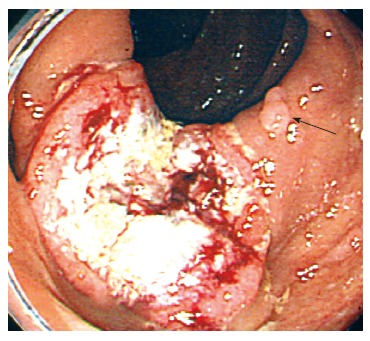
We report a patient with hyperplastic polyposis who had two asynchronous colon cancers, a combined adenoma-hyperplastic polyp, a serrated adenoma, and tubular adenomas. Hyperplastic polyposis is thought to be a precancerous lesion; and adenocarcinoma arises from hyperplastic polyposis through the hyperplastic polyp-adenoma-carcinoma sequence. Most polyps in patients with hyperplastic polyposis present as bland-looking hyperplastic polyps, which are regarded as non-neoplastic lesions; however, the risk of malignancy should not be underestimated. In patients with multiple hyperplastic polyps, hyperplastic polyposis should be identified and followed up carefully in order to detect malignant transformation in the early stage.
Figures



Similar articles
-
Hyperplastic polyposis of the large bowel. Three cases and a review of the literature.Scand J Gastroenterol. 1996 Aug;31(8):825-30. doi: 10.3109/00365529609010360. Scand J Gastroenterol. 1996. PMID: 8858755 Review.
-
Adenomatous and carcinomatous changes within hyperplastic colonic epithelium.Dis Colon Rectum. 1979 Apr;22(3):152-6. doi: 10.1007/BF02586805. Dis Colon Rectum. 1979. PMID: 446245
-
Phenotypic and molecular characteristics of hyperplastic polyposis.Gastroenterology. 2000 Aug;119(2):323-32. doi: 10.1053/gast.2000.9361. Gastroenterology. 2000. PMID: 10930367
-
'Serrated' adenoma of the colorectum, with reference to its gastric differentiation and its malignant potential.J Pathol. 1999 Apr;187(5):511-7. doi: 10.1002/(SICI)1096-9896(199904)187:5<511::AID-PATH308>3.0.CO;2-8. J Pathol. 1999. PMID: 10398114
-
[Precancerous lesions of the colon and rectum].Gan To Kagaku Ryoho. 1984 Jan;11(1):1-9. Gan To Kagaku Ryoho. 1984. PMID: 6364991 Review. Japanese.
Cited by
-
Prophylactic colectomy for hyperplastic polyposis.Ir J Med Sci. 2011 Mar;180(1):269-70. doi: 10.1007/s11845-009-0422-5. Epub 2009 Sep 26. Ir J Med Sci. 2011. PMID: 19784713
-
Filiform polyposis in the sigmoid colon: a case series.World J Gastroenterol. 2010 May 21;16(19):2443-7. doi: 10.3748/wjg.v16.i19.2443. World J Gastroenterol. 2010. PMID: 20480534 Free PMC article.
References
-
- Burt RW, Jass JR. Hyperplastic polyposis. In: Hamilton SR, Aaltonen LA, editors. World Health Organisation classification of tumours. Pathology and genetics. Tumours of the digestive system. Berlin: Springer-Verlag; 2000. pp. 135–136.
-
- Abeyasundara H, Hampshire P. Hyperplastic polyposis associated with synchronous adenocarcinomas of the transverse colon. ANZ J Surg. 2001;71:686–687. - PubMed
-
- Sumner HW, Wasserman NF, McClain CJ. Giant hyperplastic polyposis of the colon. Dig Dis Sci. 1981;26:85–89. - PubMed
-
- Ponz de Leon M, Di Gregorio C. Pathology of colorectal cancer. Dig Liver Dis. 2001;33:372–388. - PubMed
-
- Goswami RS, Minoo P, Baker K, Chong G, Foulkes WD, Jass JR. Hyperplastic polyposis and cancer of the colon with gastrinoma of the duodenum. Nat Clin Pract Oncol. 2006;3:281–284; quiz 285. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
