

Distal pancreatectomy with en bloc celiac axis resection for locally advanced pancreatic body cancer: long-term results
- PMID: 17592290
- PMCID: PMC1899197
- DOI: 10.1097/01.sla.0000258608.52615.5a
Distal pancreatectomy with en bloc celiac axis resection for locally advanced pancreatic body cancer: long-term results
Abstract
Objective: To analyze the long-term results of distal pancreatectomy with en bloc celiac axis resection (DP-CAR), a newly designed extended surgical procedure for locally advanced cancer of the pancreatic body.
Summary background data: Pancreatic body cancer often involves the common hepatic artery and/or the celiac axis and is regarded as an unresectable disease. We previously reported the feasibility and safety of DP-CAR in 10 patients and 3 preliminary cases; however, the long-term results are unknown.
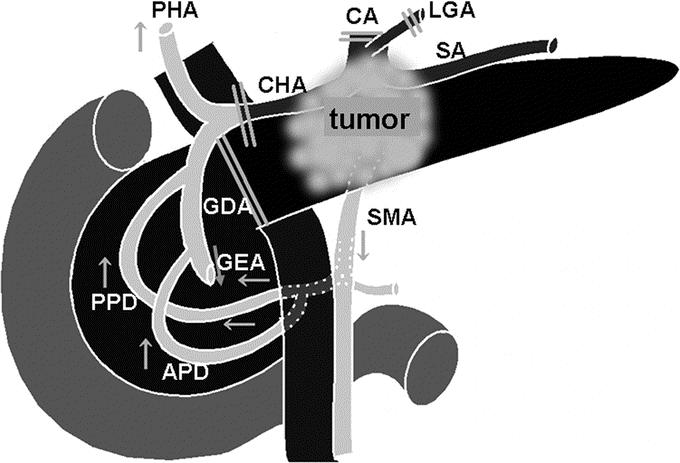
Methods: Between May 1998 and September 2005, 23 patients underwent DP-CAR. No reconstruction of the arterial system was required because of early development of the collateral arterial pathways via the pancreatoduodenal arcades from the superior mesenteric artery. We routinely used preoperative coil embolization of the common hepatic artery to enlarge the collateral pathways.
Results: The postoperative mortality rate was 0%, despite a high morbidity rate (48%). The chief postoperative complications were pancreatic fistula and ischemic gastropathy. Contrary to expectations, postoperative diarrhea was mild. Preoperative intractable abdominal and/or back pain in 10 patients was completely alleviated immediately after surgery. The surgical margins were histologically negative in 21 patients (91%). The estimated overall 1- and 5-year survival rates were 71% and 42%, respectively, and the median survival was 21.0 months. The sites of recurrence were the liver in 6 patients and local recurrence in 2.
Conclusions: DP-CAR offers a high R0 resectability rate and may potentially achieve complete local control in selected patients. The persisting early hepatic recurrence may indicate DP-CAR for the treatment of less advanced disease.
Figures




References
-
- Takahashi T, Ishikura H, Motohara T, et al. Perineural invasion by ductal adenocarcinoma of the pancreas. J Surg Oncol. 1997;65:164–170. - PubMed
-
- Takahashi S, Hasebe T, Oda T, et al. Extra-tumor perineural invasion predicts postoperative development of peritoneal dissemination in pancreatic ductal adenocarcinoma. Anticancer Res. 2001;21:1407–1412. - PubMed
-
- Kondo S, Katoh H, Shimizu T, et al. Preoperative embolization of the common hepatic artery in preparation for radical pancreatectomy for pancreas body cancer. Hepatogastroenterology. 2000;47:1447–1449. - PubMed
-
- Japan Pancreas Society. Classification of Pancreatic Carcinoma, 2nd English ed. Tokyo: Kanehara Shuppan, 2003.
-
- Yi SQ, Miwa K, Ohta T, et al. Innervation of the pancreas from the perspective of perineural invasion of pancreatic cancer. Pancreas. 2003;27:225–229. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
