

Laparoscopic distal pancreatectomy: results on a consecutive series of 58 patients
- PMID: 17592294
- PMCID: PMC1899215
- DOI: 10.1097/01.sla.0000258607.17194.2b
Laparoscopic distal pancreatectomy: results on a consecutive series of 58 patients
Abstract
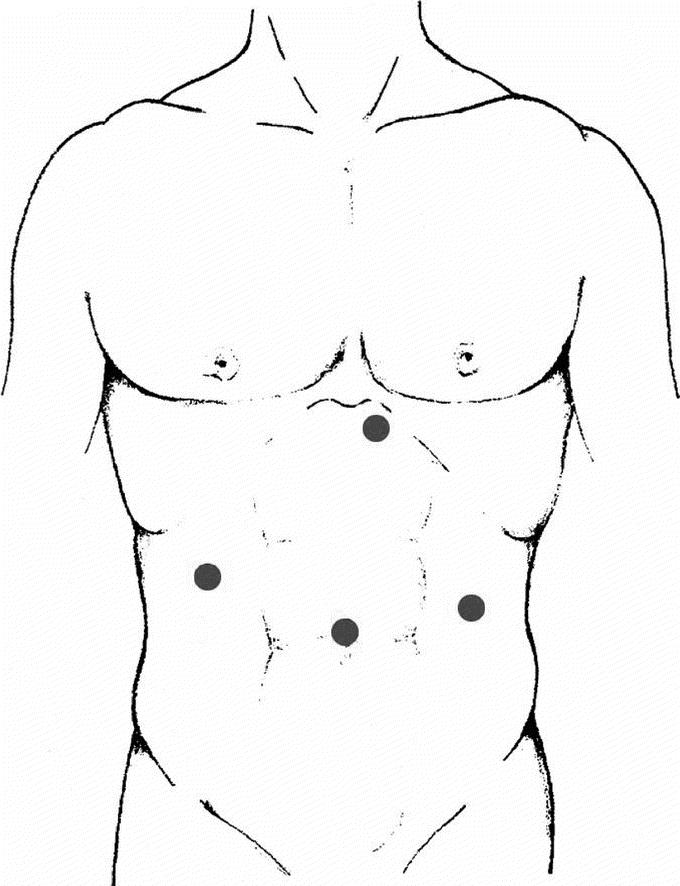
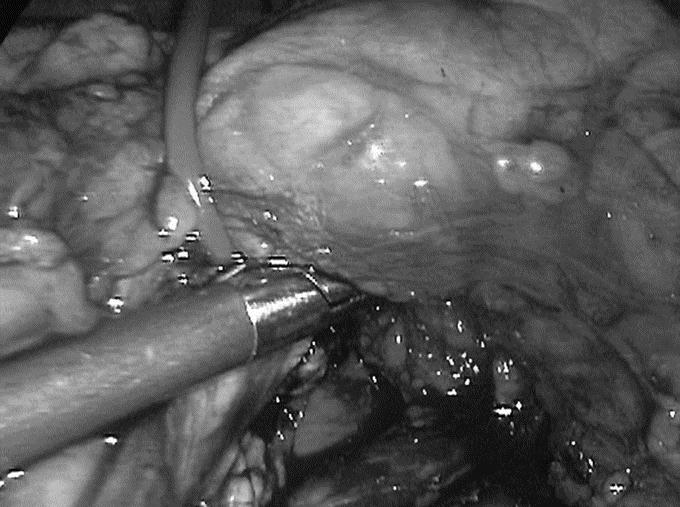
Objective: To describe the clinical characteristics, indications, technical procedures, and outcome of a consecutive series of laparoscopic distal pancreatic resections performed by the same surgical team.
Summary background data: Laparoscopic distal pancreatic resection has increasingly been described as a feasible and safe procedure, although accompanied by a high rate of conversion and morbidity.
Methods: A consecutive series of patients affected by solid and cystic tumors were selected prospectively to undergo laparoscopic distal pancreatectomy performed by the same surgical team. Clinical characteristics as well as diagnostic preoperative assessment and intra- and postoperative data were prospectively recorded. A follow-up of at least 3 months was available for all patients.
Results: Fifty-eight patients underwent laparoscopic resection between May 1999 and November 2005. All procedures were successfully performed laparoscopically, and no patient required intraoperative blood transfusion. Splenic vessel preservation was possible in 84.4% of spleen-preserving procedures. There were no mortalities. The overall median hospital stay was 9 days, while it was 10.5 days for patients with postoperative pancreatic fistulae (27.5% of all cases). Follow-up was available for all patients.
Conclusions: Our experience in 58 consecutive patients was characterized by the lack of conversions and by acceptable rates of postoperative pancreatic fistulae and morbidity. Laparoscopy proved especially beneficial in patients with postoperative complications as they had a relatively short hospital stay. Solid and cystic tumors of the distal pancreas represent a good indication for laparoscopic resection whenever possible.
Figures
References
-
- Underwood RA, Soper NJ. Current status of laparoscopic surgery of the pancreas. J Hepatobiliary Pancreat Surg. 1999;6(2):154–64. - PubMed
-
- Melotti G, Piccoli M. Pancreas e laparoscopia. Con la telecamera dove sembra impossibile. Osp Ital Chir. 2000;6:331–332.
-
- Soper NJ, Brunt LM, Dunnegan DL, et al. Laparoscopic distal pancreatectomy in the porcine model. Surg Endosc. 1994;8:57–60; Discussion 60–1. - PubMed
-
- Gagner M, Pomp A, Herrera MF. Early experience with laparoscopic resections of islet cell tumors. Surgery. 1996;120:1051–1054. - PubMed
-
- Mabrut JY, Fernandez-Cruz L, Azagra JS, et al. Laparoscopic pancreatic resection: results of a multicenter European study of 127 patients. Surgery. 2005;137:597–605. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
