

Effect of bladder filling on doses to prostate and organs at risk: a treatment planning study
- PMID: 17592448
- PMCID: PMC5722405
- DOI: 10.1120/jacmp.v8i1.2286
Effect of bladder filling on doses to prostate and organs at risk: a treatment planning study
Abstract
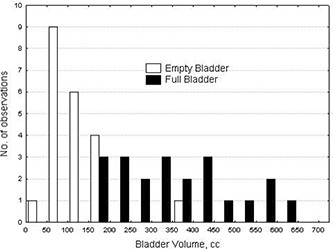
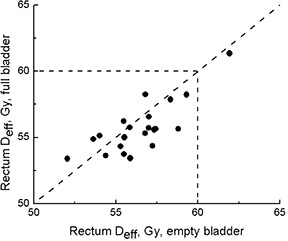
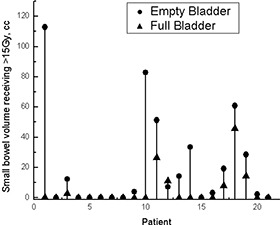
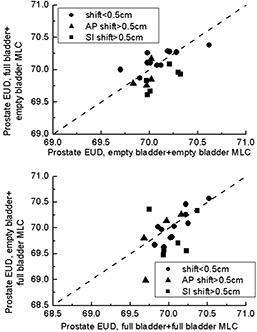
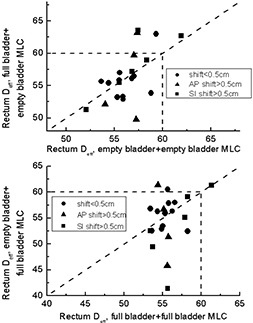
In the present study, we aimed to evaluate effects of bladder filling on dose-volume distributions for bladder, rectum, planning target volume (PTV), and prostate in radiation therapy of prostate cancer. Patients (n = 21) were scanned with a full bladder, and after 1 hour, having been allowed to void, with an empty bladder. Radiotherapy plans were generated using a four-field box technique and dose of 70 Gy in 35 fractions. First, plans obtained for full- and empty-bladder scans were compared. Second, situations in which a patient was planned on full bladder but was treated on empty bladder, and vice versa, were simulated, assuming that patients were aligned to external tattoos. Doses to the prostate [equivalent uniform dose (EUD)], bladder and rectum [effective dose (Deff)], and normal tissue complication probability (NTCP) were compared. Dose to the small bowel was examined. Mean bladder volume was 354.3 cm3 when full and 118.2 cm3 when empty. Median prostate EUD was 70 Gy for plans based on full- and empty-bladder scans alike. The median rectal Deff was 55.6 Gy for full-bladder anatomy and 56.8 Gy for empty-bladder anatomy, and the corresponding bladder Deff was 29.0 Gy and 49.3 Gy respectively. In 1 patient, part of the small bowel (7.5 cm3) received more than 50 Gy with full-bladder anatomy, and in 6 patients, part (2.5 cm3-30 cm3) received more than 50 Gy with empty-bladder anatomy. Bladder filling had no significant impact on prostate EUD or rectal Deff. A minimal volume of the small bowel received more than 50 Gy in both groups, which is below dose tolerance. The bladder Deff was higher with empty-bladder anatomy; however, the predicted complication rates were clinically insignificant. When the multileaf collimator pattern was applied in reverse, substantial underdosing of the planning target volume (PTV) was observed, particularly for patients with prostate shifts in excess of 0.5 cm in any one direction. However, the prostate shifts showed no correlation with bladder filling, and therefore the PTV underdosing also cannot be related to bladder filling. For some patients, bladder dose-volume constraints were not fulfilled in the worst-case scenario-that is, when a patient planned with full bladder consistently arrived for treatment with an empty bladder.
Figures





References
-
- Zellars RC, Roberson PL, Strawderman M, et al. Prostate position late in the course of external beam therapy: patterns and predictors. Int J Radiat Oncol Biol Phys. 2000; 47 (3): 655–660. - PubMed
-
- Melian E, Mageras GS, Fuks Z, et al. Variation in prostate position quantitation and implications for three‐dimensional conformal treatment planning. Int J Radiat Oncol Biol Phys. 1997; 38 (1): 73–81. - PubMed
-
- Schild SE, Casale HE, Bellefontaine LP. Movements of the prostate due to rectal and bladder distension: implications for radiotherapy. Med Dosim. 1993; 18 (1): 13–15. - PubMed
-
- Ten Haken RK, Forman JD, Heimburger DK, et al. Treatment planning issues related to prostate movement in response to differential filling of the rectum and bladder. Int J Radiat Oncol Biol Phys. 1991; 20 (6): 1317–1324. - PubMed
-
- Zelefsky MJ, Crean D, Mageras GS, et al. Quantification and predictors of prostate position variability in 50 patients evaluated with multiple CT scans during conformal radiotherapy. Radiother Oncol. 1999; 50 (2): 225–234. - PubMed
