

A single institutional experience of thymic epithelial tumours over 11 years: clinical features and outcome and implications for future management
- PMID: 17592498
- PMCID: PMC2359672
- DOI: 10.1038/sj.bjc.6603833
A single institutional experience of thymic epithelial tumours over 11 years: clinical features and outcome and implications for future management
Abstract
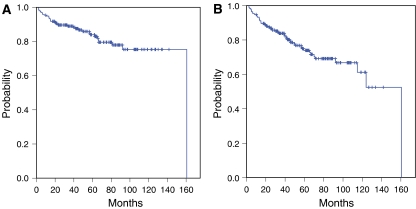
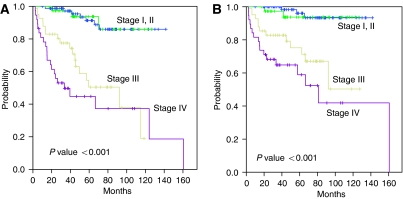
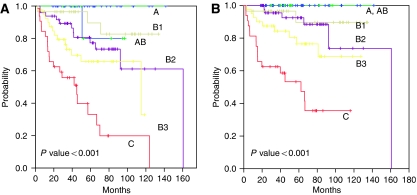
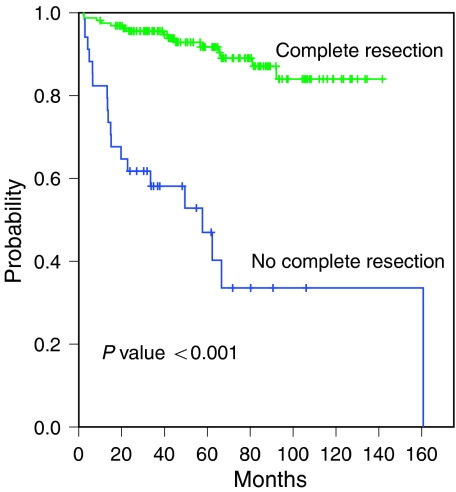
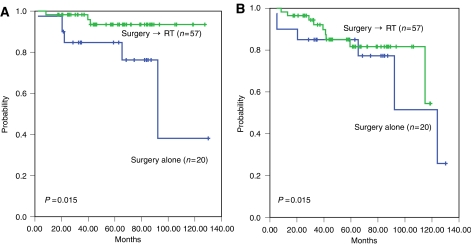
Thymic epithelial tumours (TETs), the most common tumour of the anterior mediastinum, are epithelial neoplasms of the thymus with a wide spectrum of morphologic features. We retrospectively analysed clinical features of TET and the correlation of World Health Organisation (WHO) histologic classification and Masaoka staging system with different treatment modalities in 195 patients, from 1995 to 2005. According to the Masaoka's staging system, there were 78 (40.0 %) patients with stage I, 38 (19.5%) with stage II, 41 (21.0%) with stage III, 38 (19.5%) with stage IV. All patients were reclassified according to the WHO criteria as follows: Type A (n=9, 4.6%), AB (n=37, 18.9%), B1 (n=29, 14.8%), B2 (n=48, 24.6%), B3 (n=40, 20.5%), C (n=32, 16.4%). There was a fairly good correlation between Masaoka staging and WHO histotype (P<0.05). However, in multivariate analysis, the tumour stage and WHO histotype were two independent factors separately for predicting overall survival (P<0.001, P<0.001, respectively). Thus, both Masaoka stage and WHO histotype should be considered in risk stratification of therapy for TET patients. Patients with completely resected types B2, B3 and C and adjuvant radiotherapy (n=57) had more favourable disease-free and overall survival as compared with those without adjuvant treatment (n=20) (P=0.015, 0.015, respectively). Given that the predominant sites of recurrence after surgery was pleura/pericardium and lung, and the fact that complete resection was a significant influential factor for survival at log-rank test, an active investigation of newer treatment strategies such as neoadjuvant treatment to improve the resectability and development of optimal adjuvant treatment modality is a high priority especially for those with high-risk for recurrence or in patients with advanced stage disease.
Figures
References
-
- Blumberg D, Port JL, Weksler B, Delgado R, Rosai J, Bains MS, Ginsberg RJ, Martini N, McCormack PM, Rusch V, Burt ME (1995) Thymoma: a multivariate analysis of factors predicting survival. Ann Thorac Surg 60: 908–913. discussion 914 - PubMed
-
- Chalabreysse L, Roy P, Cordier JF, Loire R, Gamondes JP, Thivolet-Bejui F (2002) Correlation of the WHO schema for the classification of thymic epithelial neoplasms with prognosis: a retrospective study of 90 tumours. Am J Surg Pathol 26: 1605–1611 - PubMed
-
- Chen G, Marx A, Wen-Hu C, Yong J, Puppe B, Stroebel P, Mueller-Hermelink HK (2002) New WHO histologic classification predicts prognosis of thymic epithelial tumours: a clinicopathologic study of 200 thymoma cases from China. Cancer 95: 420–429 - PubMed
-
- Fang W, Chen W, Chen G, Jiang Y (2005) Surgical management of thymic epithelial tumours: a retrospective review of 204 cases. Ann Thorac Surg 80: 2002–2007 - PubMed
-
- Hsu CP, Chen CY, Chen CL, Lin CT, Hsu NY, Wang JH, Wang PY (1994) Thymic carcinoma. Ten years’ experience in twenty patients. J Thorac Cardiovasc Surg 107: 615–620 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
