

A network model to predict the risk of death in sickle cell disease
- PMID: 17600133
- PMCID: PMC1988954
- DOI: 10.1182/blood-2007-04-084921
A network model to predict the risk of death in sickle cell disease
Abstract
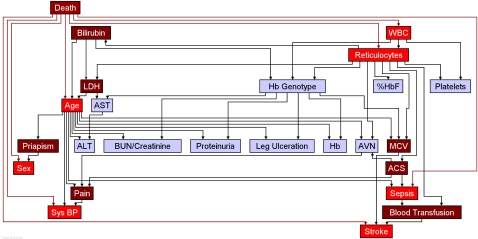
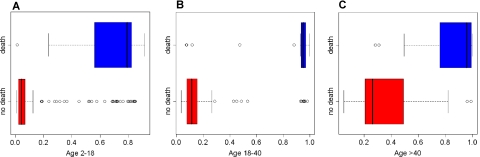
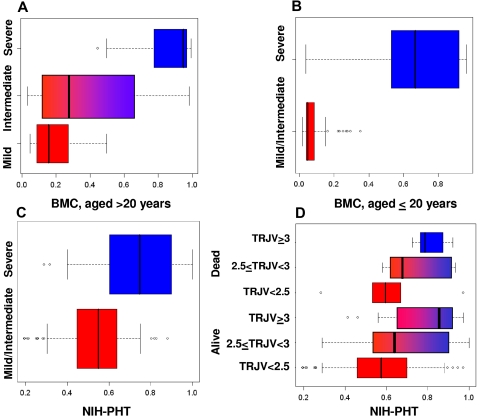
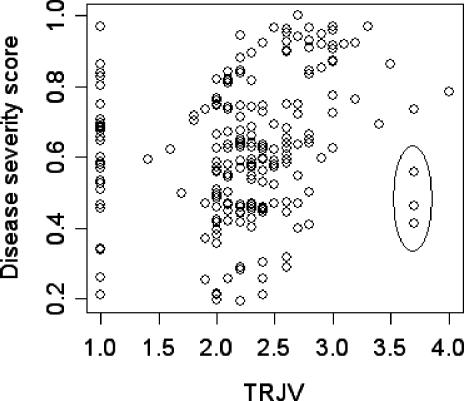
Modeling the complexity of sickle cell disease pathophysiology and severity is difficult. Using data from 3380 patients accounting for all common genotypes of sickle cell disease, Bayesian network modeling of 25 clinical events and laboratory tests was used to estimate sickle cell disease severity, which was represented as a score predicting the risk of death within 5 years. The reliability of the model was supported by analysis of 2 independent patient groups. In 1 group, the severity score was related to disease severity based on the opinion of expert clinicians. In the other group, the severity score was related to the presence and severity of pulmonary hypertension and the risk of death. Along with previously known risk factors for mortality, like renal insufficiency and leukocytosis, the network identified laboratory markers of the severity of hemolytic anemia and its associated clinical events as contributing risk factors. This model can be used to compute a personalized disease severity score allowing therapeutic decisions to be made according to the prognosis. The severity score could serve as an estimate of overall disease severity in genotype-phenotype association studies, and the model provides an additional method to study the complex pathophysiology of sickle cell disease.
Figures
Comment in
-
Usefulness and limitations of Bayesian network model as a mortality risk assessment tool in sickle cell anemia.Am J Hematol. 2009 May;84(5):312-3. doi: 10.1002/ajh.21379. Am J Hematol. 2009. PMID: 19338040 No abstract available.
References
-
- Frempong KO, Steinberg MH. Clinical aspects of sickle cell anemia in adults and children. In: Steinberg MH, Forget BG, Higgs DR, Nagel RL, editors. Disorders of Hemoglobin: Genetics, Pathophysiology, and Clinical Management. 1st ed. Cambridge, England: Cambridge University Press; 2001. pp. 611–670.
-
- Stuart MJ, Nagel RL. Sickle-cell disease. Lancet. 2004;364:1343–1360. - PubMed
-
- Platt OS, Brambilla DJ, Rosse WF, et al. Mortality in sickle cell disease: life expectancy and risk factors for early death. N Engl J Med. 1994;330:1639–1644. - PubMed
-
- Steinberg MH, Dreiling BJ, Morrison FS, Necheles TF. Mild sickle cell disease: clinical and laboratory studies. JAMA. 1973;224:317–321. - PubMed
-
- Odenheimer DJ, Sarnaik SA, Whitten CF, Rucknagel DL, Sing CF. The relationship between fetal hemoglobin and disease severity in children with sickle cell anemia. Am J Med Genet. 1987;27:525–535. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
