

Clinical review: allocating ventilators during large-scale disasters--problems, planning, and process
- PMID: 17601354
- PMCID: PMC2206420
- DOI: 10.1186/cc5929
Clinical review: allocating ventilators during large-scale disasters--problems, planning, and process
Abstract
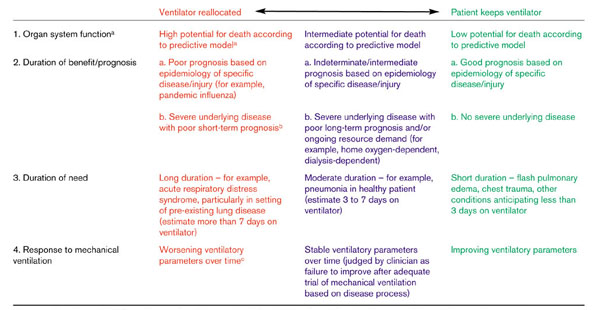
Catastrophic disasters, particularly a pandemic of influenza, may force difficult allocation decisions when demand for mechanical ventilation greatly exceeds available resources. These situations demand integrated incident management responses on the part of the health care facility and community, including resource management, provider liability protection, community education and information, and health care facility decision-making processes designed to allocate resources as justly as possible. If inadequate resources are available despite optimal incident management, a process that is evidence-based and as objective as possible should be used to allocate ventilators. The process and decision tools should be codified pre-event by the local and regional healthcare entities, public health agencies, and the community. A proposed decision tool uses predictive scoring systems, disease-specific prognostic factors, response to current mechanical ventilation, duration of current and expected therapies, and underlying disease states to guide decisions about which patients will receive mechanical ventilation. Although research in the specifics of the decision tools remains nascent, critical care physicians are urged to work with their health care facilities, public health agencies, and communities to ensure that a just and clinically sound systematic approach to these situations is in place prior to their occurrence.
Figures
Similar articles
-
Concept of operations for triage of mechanical ventilation in an epidemic.Acad Emerg Med. 2006 Feb;13(2):223-9. doi: 10.1197/j.aem.2005.07.037. Epub 2006 Jan 6. Acad Emerg Med. 2006. PMID: 16400088
-
Priority setting and the ethics of resource allocation within VA healthcare facilities: results of a survey.Organ Ethic. 2008 Fall-Winter;4(2):83-96. Organ Ethic. 2008. PMID: 18839751
-
Community planning for pandemic influenza: lessons from the VA health care system.Disaster Med Public Health Prep. 2008 Dec;2(4):251-7. doi: 10.1097/DMP.0b013e31817dd143. Disaster Med Public Health Prep. 2008. PMID: 18824920
-
An influenza pandemic exercise in a major urban setting, Part I: Hospital health systems lessons learned and implications for future planning.Am J Disaster Med. 2009 Mar-Apr;4(2):120-8. Am J Disaster Med. 2009. PMID: 19522130 Review.
-
Too Many Patients…A Framework to Guide Statewide Allocation of Scarce Mechanical Ventilation During Disasters.Chest. 2019 Apr;155(4):848-854. doi: 10.1016/j.chest.2018.09.025. Epub 2018 Oct 11. Chest. 2019. PMID: 30316913 Review.
Cited by
-
Utstein-style template for uniform data reporting of acute medical response in disasters.PLoS Curr. 2012 Mar 23;4:e4f6cf3e8df15a. doi: 10.1371/4f6cf3e8df15a. PLoS Curr. 2012. PMID: 23066513 Free PMC article.
-
The Simple Triage Scoring System (STSS) successfully predicts mortality and critical care resource utilization in H1N1 pandemic flu: a retrospective analysis.Crit Care. 2011;15(1):R39. doi: 10.1186/cc10001. Epub 2011 Jan 26. Crit Care. 2011. PMID: 21269458 Free PMC article.
-
Altered standards of care during an influenza pandemic: identifying ethical, legal, and practical principles to guide decision making.Disaster Med Public Health Prep. 2009 Dec;3 Suppl 2(Suppl 2):S132-40. doi: 10.1097/DMP.0b013e3181ac3dd2. Disaster Med Public Health Prep. 2009. PMID: 19755912 Free PMC article.
-
"We're Not Ready, But I Don't Think You're Ever Ready." Clinician Perspectives on Implementation of Crisis Standards of Care.AJOB Empir Bioeth. 2020 Jul-Sep;11(3):148-159. doi: 10.1080/23294515.2020.1759731. Epub 2020 May 5. AJOB Empir Bioeth. 2020. PMID: 32369433 Free PMC article.
-
Practices in Triage and Transfer of Critically Ill Patients: A Qualitative Systematic Review of Selection Criteria.Crit Care Med. 2020 Nov;48(11):e1147-e1157. doi: 10.1097/CCM.0000000000004624. Crit Care Med. 2020. PMID: 32858530 Free PMC article.
References
-
- Critical Care Units: A Descriptive Analysis 3-1-2005. Des Plaines, IL: Society of Critical Care Medicine; 2005.
-
- Rubinson L, Nuzzo JB, Talmor DS, O'Toole T, Kramer BR, Inglesby TV. Augmentation of hospital critical care capacity after bioterrorist attacks or epidemics: recommendations of the Working Group on Emergency Mass Critical Care. Crit Care Med. 2005;33:2393–2403. doi: 10.1097/01.CCM.0000173411.06574.D5. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
