

Microvascular reconstruction of the skull base: a clinical approach to surgical defect classification and flap selection
- PMID: 17603640
- PMCID: PMC1852578
- DOI: 10.1055/s-2006-959331
Microvascular reconstruction of the skull base: a clinical approach to surgical defect classification and flap selection
Abstract
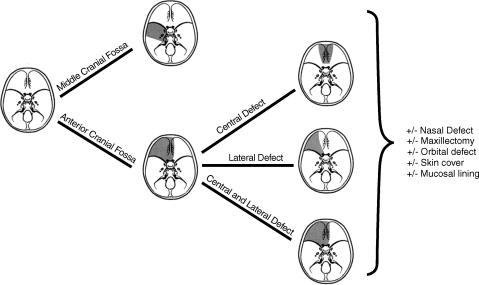
Skull-base tumor resection and reconstruction produce a major physiologic and anatomic impact on the patient. At our institution, the use of vascularized, free-tissue transfer has replaced pedicled flaps as the preferred modality for reconstructing complex cranial base defects involving resection of dura, brain, or multiple major structures adjacent to skull base, including the orbit, palate, mandible, skin, and other structures. The goals of reconstruction are to: (1) support the brain and orbit; (2) separate the CNS from the aerodigestive tract; (3) provide lining for the nasal cavity; (4) re-establish the nasal and oropharyngeal cavities; (5) provide volume to decrease dead space; and (6) restore the three-dimensional appearance of the face and head with bone and soft tissues. Surgical management requires a multidisciplinary effort with collaborating neurosurgical, head and neck, and plastic surgical teams. Successful reconstruction of skull base defects is predicated upon a careful appreciation of the specific region. Defects may be classified based on their anatomic location and loss of volume, support, and skin cover. Free flaps provide reliable, well-vascularized soft tissue to seal the dura, obliterate dead space, cover exposed cranial bone, and provide cutaneous coverage for skin or mucosa.
Figures




Similar articles
-
Anterior cranial base reconstruction using free tissue transfer: changing trends.Head Neck. 2003 Feb;25(2):89-96. doi: 10.1002/hed.10179. Head Neck. 2003. PMID: 12509790
-
Successful reconstruction of irradiated anterior skull base defect using the dual flap technique involving local pericranial flap and radial forearm free flap.J Craniofac Surg. 2014 Jul;25(4):1376-8. doi: 10.1097/SCS.0000000000000858. J Craniofac Surg. 2014. PMID: 24902109
-
Microvascular reconstruction of the skull base.Semin Surg Oncol. 2000 Oct-Nov;19(3):211-7. doi: 10.1002/1098-2388(200010/11)19:3<211::aid-ssu2>3.0.co;2-8. Semin Surg Oncol. 2000. PMID: 11135477 Review.
-
Anterior Cranial Base Reconstruction in Complex Craniomaxillofacial Trauma: An Algorithmic Approach and Single-Surgeon's Experience.Arch Plast Surg. 2022 Apr 6;49(2):174-183. doi: 10.1055/s-0042-1744406. eCollection 2022 Mar. Arch Plast Surg. 2022. PMID: 35832671 Free PMC article.
-
Reconstruction of skull base defects.Clin Plast Surg. 2005 Jul;32(3):391-9, vii. doi: 10.1016/j.cps.2005.02.001. Clin Plast Surg. 2005. PMID: 15979477 Review.
Cited by
-
Vascular pedicled flaps for skull base defect reconstruction.Laryngoscope Investig Otolaryngol. 2020 Oct 15;5(6):1029-1038. doi: 10.1002/lio2.471. eCollection 2020 Dec. Laryngoscope Investig Otolaryngol. 2020. PMID: 33364390 Free PMC article. Review.
-
A new concept for classifying skull base defects for reconstructive surgery.J Neurol Surg B Skull Base. 2012 Apr;73(2):125-31. doi: 10.1055/s-0032-1301402. J Neurol Surg B Skull Base. 2012. PMID: 23543797 Free PMC article.
-
Reconstruction of osteomyelitis defects of the craniofacial skeleton.Semin Plast Surg. 2009 May;23(2):119-31. doi: 10.1055/s-0029-1214164. Semin Plast Surg. 2009. PMID: 20567734 Free PMC article.
-
A comparison of healing and complication rates between common flaps utilized in total knee arthroplasty: a review of the literature.Knee Surg Relat Res. 2022 Mar 26;34(1):15. doi: 10.1186/s43019-022-00145-3. Knee Surg Relat Res. 2022. PMID: 35346398 Free PMC article. Review.
-
Free flap transfer in cranio-maxillofacial surgery: a review of the current data.Oral Maxillofac Surg. 2008 Sep;12(3):113-24. doi: 10.1007/s10006-008-0112-x. Oral Maxillofac Surg. 2008. PMID: 18575905 Review.
References
-
- Shah J P, Patel S G. In: Shah JP, Patel SG, editor. Head and Neck Surgery and Oncology. 3rd ed. Edinburgh, Scotland: Mosby; 2003. The skull base. pp. 93–96.
-
- Ganly I, Patel S G, Singh B, et al. Complications of craniofacial resection for malignant tumors of the skull base: report of an International Collaborative Study. Head Neck. 2005;27:445–451. - PubMed
-
- Ketcham A S, Buren J M Van. Tumors of the paranasal sinuses: a therapeutic challenge. Am J Surg. 1985;150:406–413. - PubMed
-
- Irish J C, Gullane P J, Gentili F, et al. Tumors of the skull base: outcome and survival analysis of 77 cases. Head Neck. 1994;16:3–10. - PubMed
-
- Janecka I P, Sen C, Sekhar L N, et al. Cranial base surgery: results in 183 patients. Otolaryngol Head Neck Surg. 1994;110:539–546. - PubMed
