

Age-adjusted Plasmodium falciparum antibody levels in school-aged children are a stable marker of microgeographical variations in exposure to Plasmodium infection
- PMID: 17603885
- PMCID: PMC1947991
- DOI: 10.1186/1471-2334-7-67
Age-adjusted Plasmodium falciparum antibody levels in school-aged children are a stable marker of microgeographical variations in exposure to Plasmodium infection
Abstract
Background: Amongst school-aged children living in malaria endemic areas, chronic morbidity and exacerbation of morbidity associated with other infections are often not coincident with the presence or levels of Plasmodium parasitaemia, but may result from long-term exposure to the parasite. Studies of hepatosplenomegaly associated with Schistosoma mansoni infection and exposure to Plasmodium infection indicate that differences that occur over 1-2 km in levels of Plasmodium transmission are related to the degree of exacerbation of hepatosplenomegaly and that Plasmodium falciparum schizont antigen (Pfs)-IgG3 levels may be a marker for the differing levels of exposure.
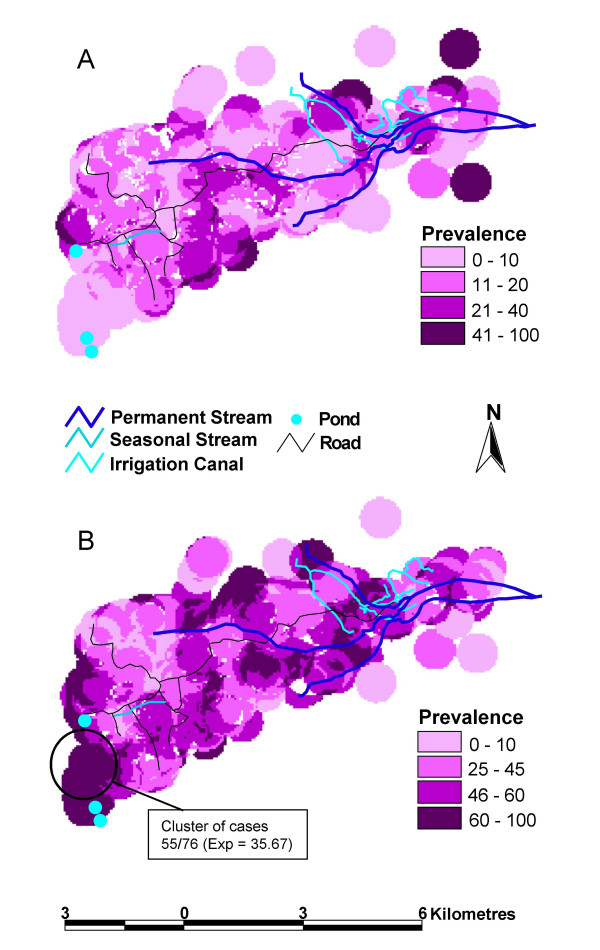
Methods: To investigate the validity of Pfs-IgG3 measurements as a tool to assess these comparative exposure levels on a microgeographical scale, cross-sectional community surveys were conducted over a 10 x 6 km study site in Makueni District, Kenya, during low and high malaria transmission seasons. During both high and low malaria transmission seasons, thick blood smears were examined microscopically and circulating Pfs-IgG3 levels measured from dried blood spot elute. GIS techniques were used to map prevalence of parasitaemia and Pfs-IgG3 levels.
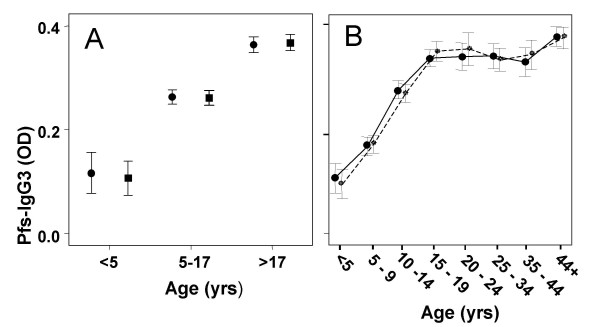
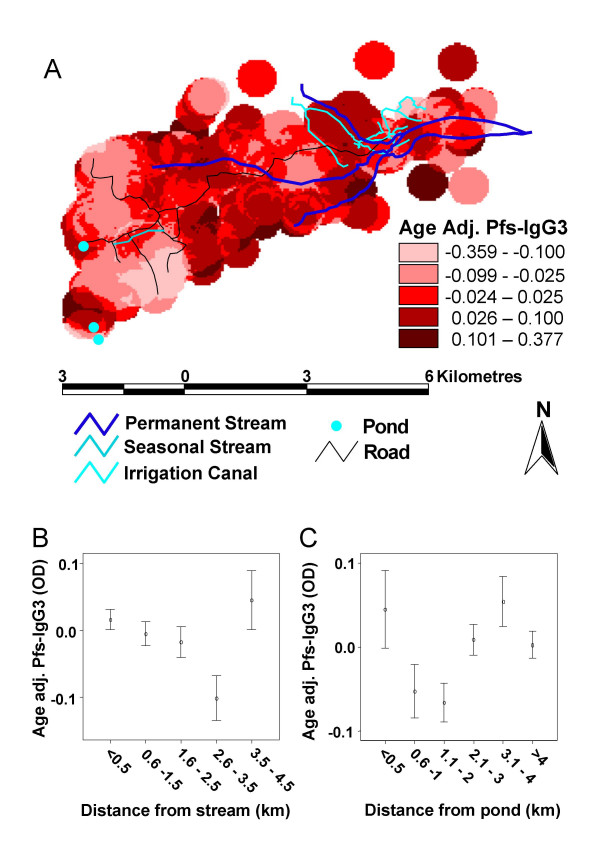
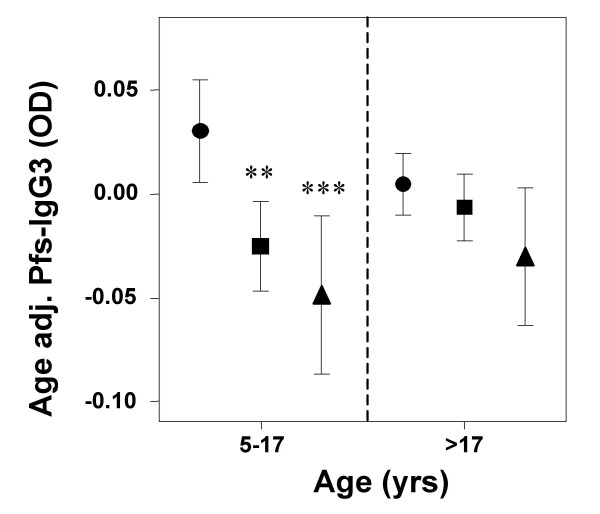
Results: Microgeographical variations in prevalence of parasitaemia were observed during the high but not the low transmission season. Pfs-IgG3 levels were stable between high and low transmission seasons, but increased with age throughout childhood before reaching a plateau in adults. Adjusting Pfs-IgG3 levels of school-aged children for age prior to mapping resulted in spatial patterns that reflected the microgeographical variations observed for high season prevalence of parasitaemia, however, Pfs-IgG3 levels of adults did not. The distances over which age-adjusted Pfs-IgG3 of school-aged children fluctuated were comparable with those distances over which chronic morbidity has previous been shown to vary.
Conclusion: Age-adjusted Pfs-IgG3 levels of school-aged children are stable and when mapped can provide a tool sensitive enough to detect microgeographical variations in malaria exposure, that would be useful for studying the aetiology of morbidities associated with long-term exposure and co-infections.
Figures
Similar articles
-
Micro-geographical variation in exposure to Schistosoma mansoni and malaria, and exacerbation of splenomegaly in Kenyan school-aged children.BMC Infect Dis. 2004 May 17;4:13. doi: 10.1186/1471-2334-4-13. BMC Infect Dis. 2004. PMID: 15147584 Free PMC article.
-
Serological responses among individuals in areas where both schistosomiasis and malaria are endemic: cross-reactivity between Schistosoma mansoni and Plasmodium falciparum.J Infect Dis. 2003 Apr 15;187(8):1272-82. doi: 10.1086/368361. Epub 2003 Apr 2. J Infect Dis. 2003. PMID: 12696007
-
Effect of transmission intensity and age on subclass antibody responses to Plasmodium falciparum pre-erythrocytic and blood-stage antigens.Acta Trop. 2015 Feb;142:47-56. doi: 10.1016/j.actatropica.2014.10.011. Epub 2014 Oct 24. Acta Trop. 2015. PMID: 25446174 Free PMC article.
-
Associations between anti-Schistosoma mansoni and anti-Plasmodium falciparum antibody responses and hepatosplenomegaly, in Kenyan schoolchildren.J Infect Dis. 2003 Apr 15;187(8):1337-41. doi: 10.1086/368362. Epub 2003 Apr 2. J Infect Dis. 2003. PMID: 12696017
-
IgG3 antibodies to Plasmodium falciparum merozoite surface protein 2 (MSP2): increasing prevalence with age and association with clinical immunity to malaria.Am J Trop Med Hyg. 1998 Apr;58(4):406-13. doi: 10.4269/ajtmh.1998.58.406. Am J Trop Med Hyg. 1998. PMID: 9574783
Cited by
-
Antibody Profiles to P. falciparum Antigens Over Time Characterize Acute and Long-Term Malaria Exposure in an Area of Low and Unstable Transmission.Am J Trop Med Hyg. 2020 Dec;103(6):2189-2197. doi: 10.4269/ajtmh.19-0480. Epub 2020 Oct 27. Am J Trop Med Hyg. 2020. PMID: 33124539 Free PMC article.
-
Marked variation in MSP-119 antibody responses to malaria in western Kenyan highlands.BMC Infect Dis. 2012 Mar 1;12:50. doi: 10.1186/1471-2334-12-50. BMC Infect Dis. 2012. PMID: 22380785 Free PMC article.
-
Health implications of chronic hepatosplenomegaly in Kenyan school-aged children chronically exposed to malarial infections and Schistosoma mansoni.Trans R Soc Trop Med Hyg. 2010 Feb;104(2):110-6. doi: 10.1016/j.trstmh.2009.08.006. Epub 2009 Oct 8. Trans R Soc Trop Med Hyg. 2010. PMID: 19818465 Free PMC article.
-
Opportunities for improved surveillance and control of dengue from age-specific case data.Elife. 2019 May 23;8:e45474. doi: 10.7554/eLife.45474. Elife. 2019. PMID: 31120419 Free PMC article.
-
Application of Serological Tools and Spatial Analysis to Investigate Malaria Transmission Dynamics in Highland Areas of Southwest Uganda.Am J Trop Med Hyg. 2016 Jun 1;94(6):1251-1258. doi: 10.4269/ajtmh.15-0653. Epub 2016 Mar 28. Am J Trop Med Hyg. 2016. PMID: 27022156 Free PMC article.
References
-
- Walters JH, Waterlow JC. Fibrosis of the liver in West African children. Spec Rep Ser Med Res Counc (G B) 1954;285:1–71. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
