

Accuracy of diagnosing atrial fibrillation on electrocardiogram by primary care practitioners and interpretative diagnostic software: analysis of data from screening for atrial fibrillation in the elderly (SAFE) trial
- PMID: 17604299
- PMCID: PMC1952490
- DOI: 10.1136/bmj.39227.551713.AE
Accuracy of diagnosing atrial fibrillation on electrocardiogram by primary care practitioners and interpretative diagnostic software: analysis of data from screening for atrial fibrillation in the elderly (SAFE) trial
Abstract
Objective: To assess the accuracy of general practitioners, practice nurses, and interpretative software in the use of different types of electrocardiogram to diagnose atrial fibrillation.
Design: Prospective comparison with reference standard of assessment of electrocardiograms by two independent specialists.
Setting: 49 general practices in central England.
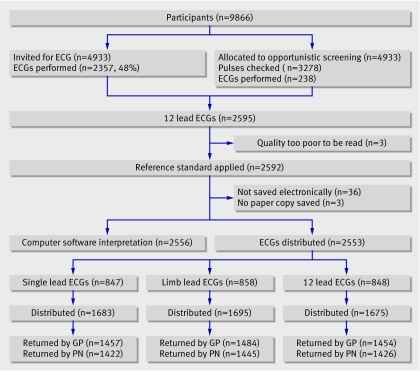
Participants: 2595 patients aged 65 or over screened for atrial fibrillation as part of the screening for atrial fibrillation in the elderly (SAFE) study; 49 general practitioners and 49 practice nurses.
Interventions: All electrocardiograms were read with the Biolog interpretative software, and a random sample of 12 lead, limb lead, and single lead thoracic placement electrocardiograms were assessed by general practitioners and practice nurses independently of each other and of the Biolog assessment.
Main outcome measures: Sensitivity, specificity, and positive and negative predictive values.
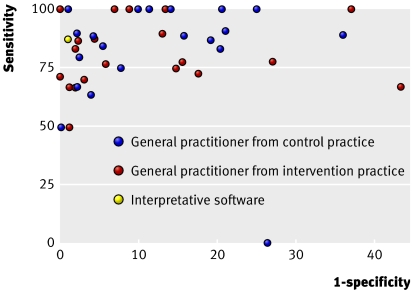
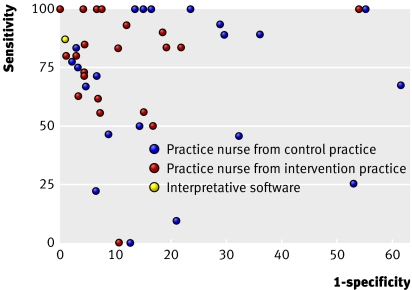
Results: General practitioners detected 79 out of 99 cases of atrial fibrillation on a 12 lead electrocardiogram (sensitivity 80%, 95% confidence interval 71% to 87%) and misinterpreted 114 out of 1355 cases of sinus rhythm as atrial fibrillation (specificity 92%, 90% to 93%). Practice nurses detected a similar proportion of cases of atrial fibrillation (sensitivity 77%, 67% to 85%), but had a lower specificity (85%, 83% to 87%). The interpretative software was significantly more accurate, with a specificity of 99%, but missed 36 of 215 cases of atrial fibrillation (sensitivity 83%). Combining general practitioners' interpretation with the interpretative software led to a sensitivity of 92% and a specificity of 91%. Use of limb lead or single lead thoracic placement electrocardiograms resulted in some loss of specificity.
Conclusions: Many primary care professionals cannot accurately detect atrial fibrillation on an electrocardiogram, and interpretative software is not sufficiently accurate to circumvent this problem, even when combined with interpretation by a general practitioner. Diagnosis of atrial fibrillation in the community needs to factor in the reading of electrocardiograms by appropriately trained people.
Conflict of interest statement
Figures
Comment in
-
Diagnosing atrial fibrillation in general practice.BMJ. 2007 Aug 25;335(7616):355-6. doi: 10.1136/bmj.39266.497396.BE. BMJ. 2007. PMID: 17717334 Free PMC article.
-
Accuracy of ECG interpretation in primary care was limited for detecting atrial fibrillation.Evid Based Med. 2008 Apr;13(2):58. doi: 10.1136/ebm.13.2.58. Evid Based Med. 2008. PMID: 18375711 No abstract available.
References
-
- Sudlow S, Thomson R, Thwaites B, Rodgers H, Kenny RA. Prevalence of atrial fibrillation and eligibility for anticoagulants in the community. Lancet 1998;352:1167-71. - PubMed
-
- Lip GYH, Edwards SJ. Stroke prevention with aspirin, warfarin and ximelagatran in patients with non-valvular atrial fibrillation: a systematic review and meta-analysis. Thromb Res 2006;118:321-33. - PubMed
-
- Salerno SM, Alguire PC, Waxman HS. Competency in interpretation of 12-lead electrocardiograms: summary and appraisal of published evidence. Ann Intern Med 2003;138:751-60. - PubMed
-
- Poon K, Okin P, Kligfield P. Diagnostic performance of a computer based ECG rhythm algorithm. J Electrocardiol 2005;38:235-8. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical