Family-based obesity treatment, then and now: twenty-five years of pediatric obesity treatment
- PMID: 17605557
- PMCID: PMC2387251
- DOI: 10.1037/0278-6133.26.4.381
Family-based obesity treatment, then and now: twenty-five years of pediatric obesity treatment
Abstract
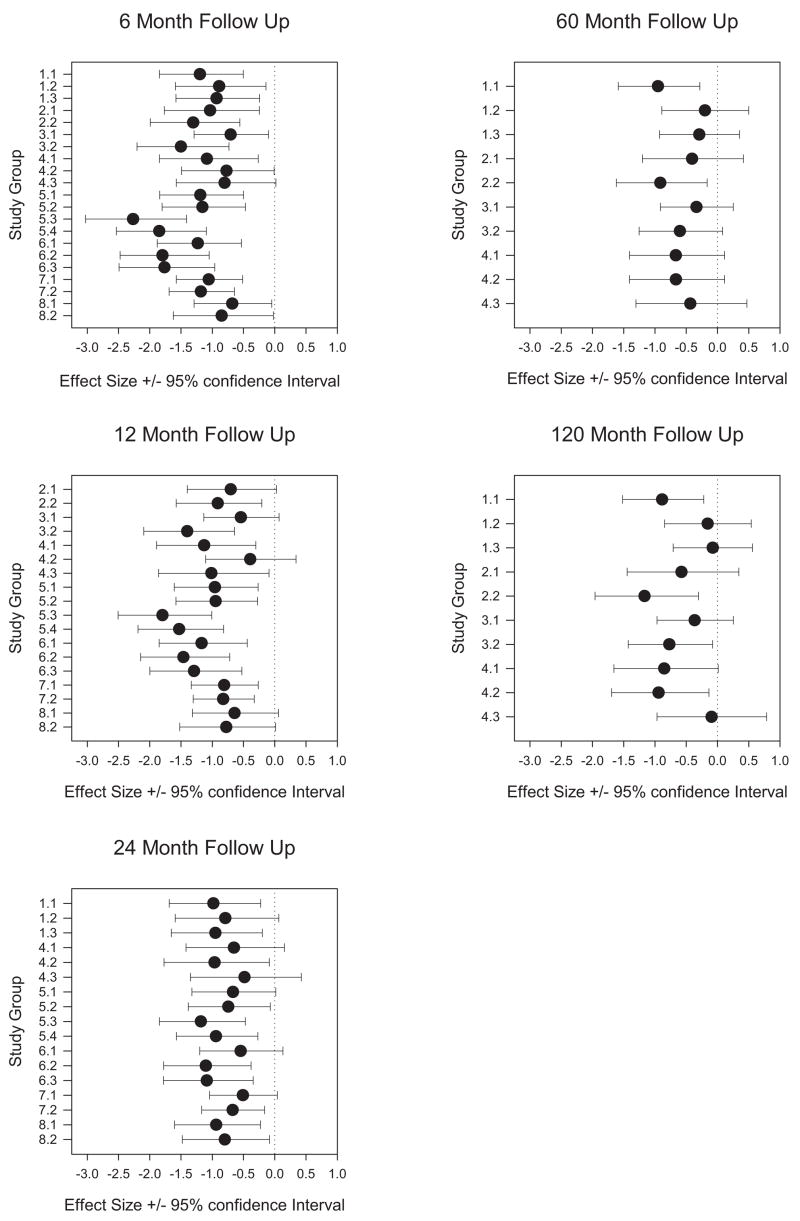
Objective: Family-based treatments for pediatric obesity were developed over 25 years ago. Over that time, youth have become more obese and the environment more obesiogenic, which may influence efficacy of pediatric weight control. Mixed-effects regression models were used to compare the efficacy of programs initiated 20 to 25 years ago to current programs through 24-month follow-up, as well as to reanalyze 10-year outcomes of previous research using contemporary measures and analytic strategies.
Main outcome measures: z-BMI and percent overweight.
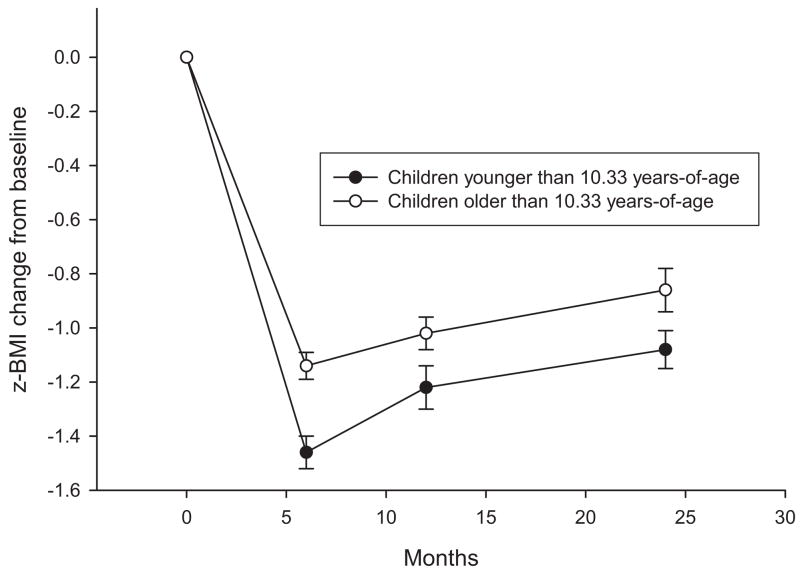
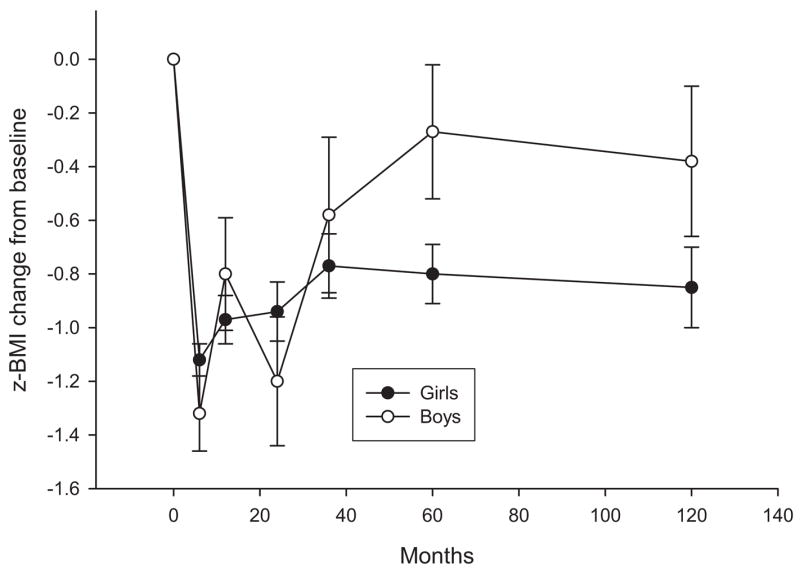
Results: Results showed significant reductions over time, with no differences in z-BMI change for older versus contemporary studies. Age was a predictor of z-BMI up to 24 months, with younger children showing larger change. Mixed-effects regression models replicated previous long-term effects of family-based interventions. Gender was a predictor of long-term z-BMI change, with girls benefiting more over time than did boys.
Conclusion: The efficacy of the family-based behavioral approach to treating pediatric obesity replicates over a 25-year period. Challenges in evaluating treatment effects over time are discussed. Ideas for studying choice of treatments that vary in effect size and for strengthening family-based behavioral treatments are noted.
Copyright 2007 APA.
Figures
References
-
- Anderson PM, Butcher KF. Childhood obesity: Trends and potential causes. Future of Children. 2006;16:19–45. - PubMed
-
- Armstrong K, Schwartz JS, Fitzgerald G, Putt M, Ubel PA. Effect of framing as gain versus loss on understanding and hypothetical treatment choices: Survival and mortality curves. Medical Decision Making. 2002;22:76–83. - PubMed
-
- Berkowitz RI, Wadden TA, Tershakovec AM, Cronquist JL. Behavior therapy and sibutramine for the treatment of adolescent obesity: A randomized controlled trial. Journal of the American Medical Association. 2003;289:1805–1812. - PubMed
-
- Biing-Hwan L, Guthrie JF, Frazao E. America’s changing eating habits: Changes and consequences. Washington, DC: U.S. Department of Agriculture, Economic Research Division; 1999. Nutrient contribution of food away from home; pp. 213–242.
-
- Bowers DE. Cooking trends echo changing roles of women. Food Review. 2000;23:23–29.