

Prescription drug cost sharing: associations with medication and medical utilization and spending and health
- PMID: 17609491
- PMCID: PMC6375697
- DOI: 10.1001/jama.298.1.61
Prescription drug cost sharing: associations with medication and medical utilization and spending and health
Abstract
Context: Prescription drugs are instrumental to managing and preventing chronic disease. Recent changes in US prescription drug cost sharing could affect access to them.
Objective: To synthesize published evidence on the associations among cost-sharing features of prescription drug benefits and use of prescription drugs, use of nonpharmaceutical services, and health outcomes.
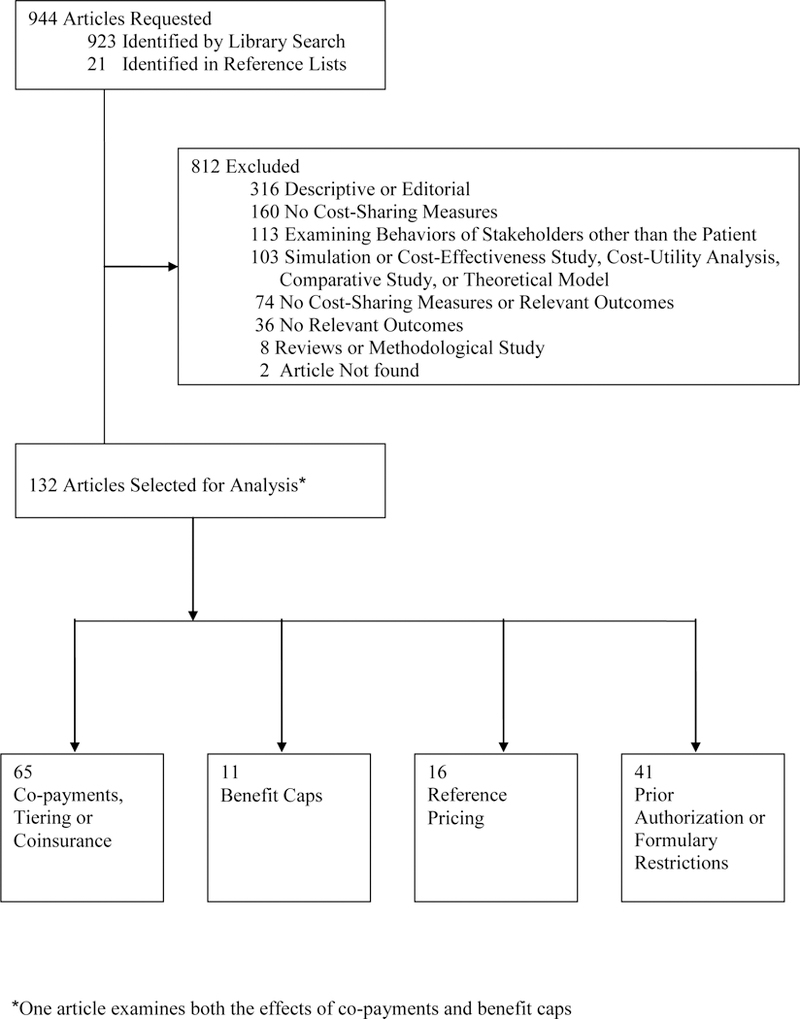
Data sources: We searched PubMed for studies published in English between 1985 and 2006.
Study selection and data extraction: Among 923 articles found in the search, we identified 132 articles examining the associations between prescription drug plan cost-containment measures, including co-payments, tiering, or coinsurance (n = 65), pharmacy benefit caps or monthly prescription limits (n = 11), formulary restrictions (n = 41), and reference pricing (n = 16), and salient outcomes, including pharmacy utilization and spending, medical care utilization and spending, and health outcomes.
Results: Increased cost sharing is associated with lower rates of drug treatment, worse adherence among existing users, and more frequent discontinuation of therapy. For each 10% increase in cost sharing, prescription drug spending decreases by 2% to 6%, depending on class of drug and condition of the patient. The reduction in use associated with a benefit cap, which limits either the coverage amount or the number of covered prescriptions, is consistent with other cost-sharing features. For some chronic conditions, higher cost sharing is associated with increased use of medical services, at least for patients with congestive heart failure, lipid disorders, diabetes, and schizophrenia. While low-income groups may be more sensitive to increased cost sharing, there is little evidence to support this contention.
Conclusions: Pharmacy benefit design represents an important public health tool for improving patient treatment and adherence. While increased cost sharing is highly correlated with reductions in pharmacy use, the long-term consequences of benefit changes on health are still uncertain.
References
-
- Lichtenberg FR. Are the benefits of newer drugs worth their cost? Evidence from the 1996 MEPS. Health Aff (Millwood) Sep-Oct 2001;20(5):241–251. - PubMed
-
- Gabel J, Levitt L, Holve E, et al. Job-based health benefits in 2002: some important trends. Health Aff (Millwood) Sep-Oct 2002;21(5):143–151. - PubMed
-
- Prescription Drug Trends Menlo Park, CA: Kaiser Family Foundation; June 2006. 3057–05.
-
- Tseng CW, Brook RH, Keeler E, Mangione CM. Impact of an annual dollar limit or “cap” on prescription drug benefits for Medicare patients. Jama July 9 2003;290(2):222–227. - PubMed
-
- Andersson K, Petzold MG, Sonesson C, Lonnroth K, Carlsten A. Do policy changes in the pharmaceutical reimbursement schedule affect drug expenditures? Interrupted time series analysis of cost, volume and cost per volume trends in Sweden 1986–2002. Health Policy December 2006;79(2–3):231–243. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
