

Is thirty-day hospital mortality really lower for black veterans compared with white veterans?
- PMID: 17610440
- PMCID: PMC1955274
- DOI: 10.1111/j.1475-6773.2006.00688.x
Is thirty-day hospital mortality really lower for black veterans compared with white veterans?
Abstract
Objective: To examine the source of observed lower risk-adjusted mortality for blacks than whites within the Veterans Affairs (VA) system by accounting for hospital site where treated, potential under-reporting of black deaths, discretion on hospital admission, quality improvement efforts, and interactions by age group.
Data sources: Data are from the VA Patient Treatment File on 406,550 hospitalizations of veterans admitted with a principal diagnosis of acute myocardial infarction, stroke, hip fracture, gastrointestinal bleeding, congestive heart failure, or pneumonia between 1996 and 2002. Information on deaths was obtained from the VA Beneficiary Identification Record Locator System and the National Death Index.
Study design: This was a retrospective observational study of hospitalizations throughout the VA system nationally. The primary outcome studied was all-location mortality within 30 days of hospital admission. The key study variable was whether a patient was black or white.
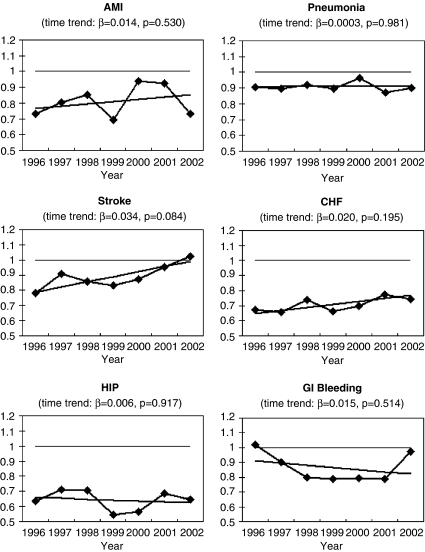
Principal findings: For each of the six study conditions, unadjusted 30-day mortality rates were significantly lower for blacks than for whites (p<.01). These results did not vary after adjusting for hospital site where treated, more complete ascertainment of deaths, and in comparing results for conditions for which hospital admission is discretionary versus non-discretionary. There were also no significant changes in the degree of difference by race in mortality by race following quality improvement efforts within VA. Risk-adjusted mortality was consistently lower for blacks than for whites only within the population of veterans over age 65.
Conclusions: Black veterans have significantly lower 30-day mortality than white veterans for six common, high severity conditions, but this is generally limited to veterans over age 65. This differential by age suggests that it is unlikely that lower 30-day mortality rates among blacks within VA are driven by treatment differences by race.
Figures
Similar articles
-
Is lower 30-day mortality posthospital admission among blacks unique to the Veterans Affairs health care system?Med Care. 2007 Nov;45(11):1083-9. doi: 10.1097/MLR.0b013e3180ca960e. Med Care. 2007. PMID: 18049349
-
Racial differences in mortality among men hospitalized in the Veterans Affairs health care system.JAMA. 2001 Jan 17;285(3):297-303. doi: 10.1001/jama.285.3.297. JAMA. 2001. PMID: 11176839
-
Short- and long-term mortality after an acute illness for elderly whites and blacks.Health Serv Res. 2008 Aug;43(4):1388-402. doi: 10.1111/j.1475-6773.2008.00837.x. Epub 2008 Mar 17. Health Serv Res. 2008. PMID: 18355259 Free PMC article.
-
Impact of race on health care utilization and outcomes in veterans with congestive heart failure.J Am Coll Cardiol. 2004 Mar 3;43(5):778-84. doi: 10.1016/j.jacc.2003.10.033. J Am Coll Cardiol. 2004. PMID: 14998616
-
The concentration of hospital care for black veterans in Veterans Affairs hospitals: implications for clinical outcomes.J Healthc Qual. 2010 Nov-Dec;32(6):52-61. doi: 10.1111/j.1945-1474.2010.00085.x. J Healthc Qual. 2010. PMID: 20946426
Cited by
-
Racial disparities in all-cause mortality among veterans with type 2 diabetes.J Gen Intern Med. 2010 Oct;25(10):1051-6. doi: 10.1007/s11606-010-1405-y. Epub 2010 Jun 8. J Gen Intern Med. 2010. PMID: 20532659 Free PMC article.
-
Trends and Racial Differences in First Hospitalization for Stroke and 30-Day Mortality in the US Medicare Population From 1988 to 2013.Med Care. 2019 Apr;57(4):262-269. doi: 10.1097/MLR.0000000000001079. Med Care. 2019. PMID: 30870384 Free PMC article.
-
Ambulance diversion and ED destination by race/ethnicity: evaluation of Massachusetts' ambulance diversion ban.BMC Health Serv Res. 2022 Aug 3;22(1):987. doi: 10.1186/s12913-022-08358-8. BMC Health Serv Res. 2022. PMID: 35918721 Free PMC article.
-
A Surgical Desirability of Outcome Ranking (DOOR) Reveals Complex Relationships Between Race/Ethnicity, Insurance Type, and Neighborhood Deprivation.Ann Surg. 2024 Feb 1;279(2):246-257. doi: 10.1097/SLA.0000000000005994. Epub 2023 Jul 14. Ann Surg. 2024. PMID: 37450703 Free PMC article.
-
Racial differences in mortality among patients with acute ischemic stroke: an observational study.Ann Intern Med. 2011 Feb 1;154(3):152-9. doi: 10.7326/0003-4819-154-3-201102010-00004. Ann Intern Med. 2011. PMID: 21282694 Free PMC article.
References
-
- Adler NE, Newman K. Socioeconomic Disparities in Health: Pathways and Policies. Health Affairs (Millwood) 2002;21(2):60–76. - PubMed
-
- Agency for Healthcare Research and Quality. AHRQ Quality Indicators—Guide to Inpatient Quality Indicators: Quality of Care in Hospitals—Volume, Mortality, and Utilization. AHRQ Pub. No. 02-R 0204. Rockville, MD: Agency for Healthcare Research and Quality; 2002.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
