

Surgical outcomes for colon and rectal cancer over a decade: results from a consecutive monocentric experience in 902 unselected patients
- PMID: 17610720
- PMCID: PMC1959229
- DOI: 10.1186/1477-7819-5-73
Surgical outcomes for colon and rectal cancer over a decade: results from a consecutive monocentric experience in 902 unselected patients
Abstract
Background: This study evaluates the surgical morbidity and long-term outcome of colorectal cancer surgery in an unselected group of patients treated over the period 1994-2003.
Methods: A consecutive series of 902 primary colorectal cancer patients (489 M, 413 F; mean age: 63 years +/- 11 years, range: 24-88 years) was evaluated and prospectively followed in a university hospital (mean follow-up 36 +/- 24 months; range: 3-108 months). Perioperative mortality, morbidity, overall survival, curative resection rates, recurrence rates were analysed.
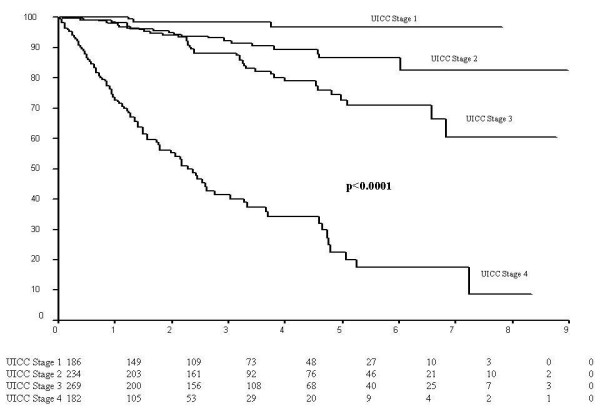
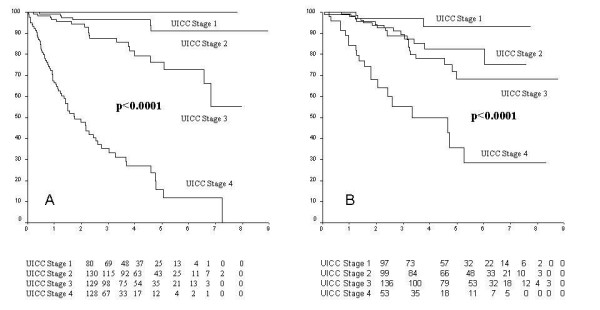
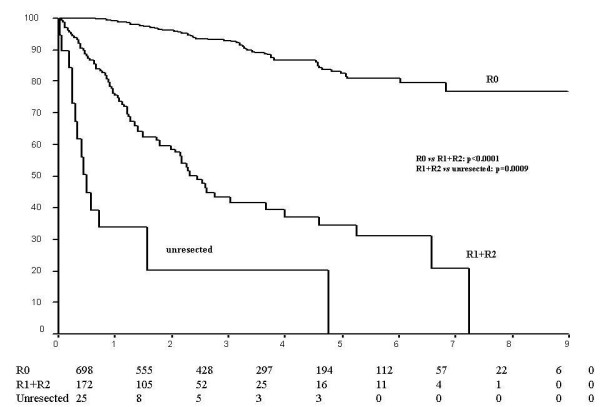
Results: Of the total, 476 colorectal cancers were localized to the colon (CC, 53%), 406 to the rectum (RC, 45%), 12 (1%) were multicentric, and 8 were identified as part of HNPCC (1%). Combining all tumours, there were 186 cancers (20.6%) defined as UICC stage I, 235 (26.1%) stage II, 270 (29.9%) stage III and 187 (20.6%) stage IV cases. Twenty-four (2.7%) cases were of undetermined stage. Postoperative complications occurred in 38% of the total group (37.8% of CC cases, 37.2% of the RC group, 66.7% of the synchronous cancer patients and 50% of those with HNPCC, p = 0.19) Mortality rate was 0.8%, (1.3% for colon cancer, 0% for rectal cancer; p = 0.023). Multivisceral resection was performed in 14.3% of cases. Disease-free survival in cases resected for cure was 73% at 5-years and 72% at 8 years. The 5- and 8-year overall survival rates were 71% and 61% respectively (total cases). At 5-year analysis, overall survival rates are 97% for stage I disease, 87% for stage II, 73% for stage III and 22% for stage IV respectively (p < 0.0001). The 5-year overall survival rates showed a marked difference in R0, R1+R2 and non resected patients (82%, 35% and 0% respectively, p < 0.0001). On multivariate analysis, resection for cure and stage at presentation but not tumour site (colon vs. rectum) were independent variables for overall survival (p < 0.0001).
Conclusion: A prospective, uniform follow-up policy used in a single institution over the last decade provides evidence of quality assurance in colorectal cancer surgery with high rates of resection for cure where only stage at presentation functions as an independent variable for cancer-related outcome.
Figures
References
-
- Hermanek P, Sobin CH, editors . 2nd rev 1992. 4. Budapest, Springer; 1993. TNM classification of malignant tumours; pp. 52–55.
-
- Hermanek P, Henson DE, Hutter RVP, Sobin CH, editors . TNM supplement 1993. Budapest, Springer; 1993. pp. 30–32. 122–124.
-
- Sobin LH, Wittekind CH, editors . TNM classification of malignant tumours. 5. New York Wiley; 1997. pp. 66–69.
-
- Beahrs OH, Henson DE, Hutter RVP, Kennedy BJ, editors . American Joint Committee on Cancer (AJCC) Manual for staging of cancer. 4. Philadelphia, Lippincott; 1992. pp. pp75–79.
-
- Fleming ID, Cooper JS, Henson DE, Hutter RVP, Kennedy PJ, Murphy GP, Sullivan PO, Sobin LH, Yarbro JW, editors . American Joint Committee on Cancer (AJCC) Cancer staging manual. 5. Philadelphia, LIPPINCOTT; 1997. pp. 83–68.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
