

Down syndrome associated with hypothyroidism and chronic pericardial effusion: echocardiographic follow-up
- PMID: 17612663
- PMCID: PMC1847750
- DOI: 10.1007/BF03085957
Down syndrome associated with hypothyroidism and chronic pericardial effusion: echocardiographic follow-up
Abstract
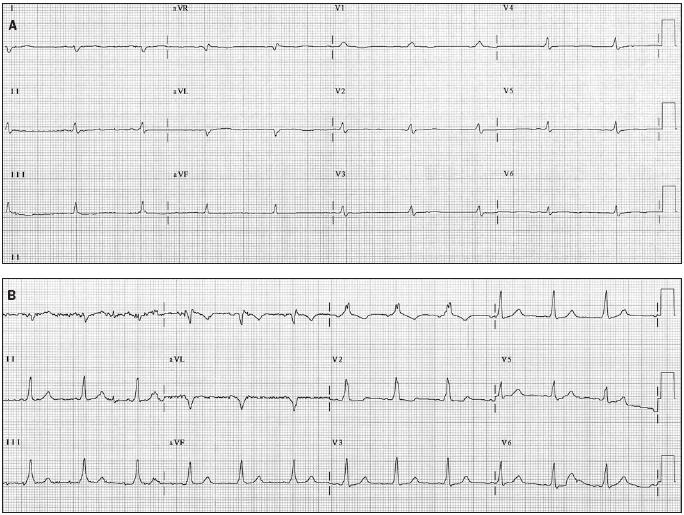
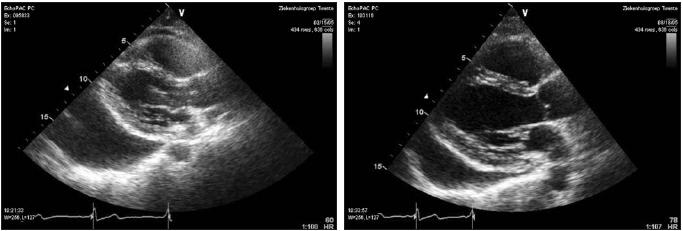
We present a 39-year-old male patient with Down syndrome who was evaluated for fatigue, palpitations and bouts of cyanosis. Physical examination showed features of trisomy-21(Down syndrome), with a slow pulse rate, distant cardiac sounds and absent apex beat. He had normal jugular venous pressure without pulsus paradoxus. The ECG showed QRS microvoltage and flattened P and T segments. The 48-hour ambulatory ECG depicted normal sinus rhythm with intermittent short PR interval without tachyarrhythmias. The chest Xray revealed cardiomegaly without pulmonary venous congestion. Although serial transthoracic echocardiographic examination demonstrated pericardial effusion with features of tamponade, there were no overt signs of clinical cardiac tamponade. Biochemically, the serum thyroxine of 3 pmol/l (normal 10 to 25) and thyroid-stimulating hormone of 160 mU/l (normal 0.20 to 4.20)) were compatible with hypothyroidism. The patient was treated with L-thyroxine sodium daily, which was gradually increased to 0.125 mg daily. Within a few months he lost weight and became more alert; furthermore, the symptoms of hypothyroidism and the pericardial effusion resolved. It can be concluded that Down syndrome may be associated with hypothyroidism and pericardial effusion. These were alleviated following hormone replacement. Regular evaluation of thyroid function tests is important in Down syndrome. (Neth Heart J 2007;15:67-70.).
Figures
Similar articles
-
Cardiac Tamponade in Down's Syndrome Associated With Hypothyroidism: An Uncommon Presentation.Cureus. 2024 Apr 25;16(4):e59023. doi: 10.7759/cureus.59023. eCollection 2024 Apr. Cureus. 2024. PMID: 38803753 Free PMC article.
-
Massive pericardial effusion and cardiac tamponade revealed undiagnosed Turner syndrome: a case report.BMC Cardiovasc Disord. 2020 Oct 23;20(1):459. doi: 10.1186/s12872-020-01728-2. BMC Cardiovasc Disord. 2020. PMID: 33096991 Free PMC article.
-
Massive pericardial effusion without cardiac tamponade due to subclinical hypothyroidism (Hashimoto's disease).Rural Remote Health. 2018 May;18(2):4384. doi: 10.22605/RRH4384. Epub 2018 May 20. Rural Remote Health. 2018. PMID: 29778090
-
Does this patient with a pericardial effusion have cardiac tamponade?JAMA. 2007 Apr 25;297(16):1810-8. doi: 10.1001/jama.297.16.1810. JAMA. 2007. PMID: 17456823 Review.
-
Cardiac tamponade. A clinical or an echocardiographic diagnosis?Circulation. 1993 May;87(5):1738-41. doi: 10.1161/01.cir.87.5.1738. Circulation. 1993. PMID: 8491026 Review.
Cited by
-
Rare complication after pericardial window: symptomatic diaphragmatic hernia containing bowel and liver.BMJ Case Rep. 2020 Nov 30;13(11):e236078. doi: 10.1136/bcr-2020-236078. BMJ Case Rep. 2020. PMID: 33257358 Free PMC article.
-
Cardiac Tamponade in Down's Syndrome Associated With Hypothyroidism: An Uncommon Presentation.Cureus. 2024 Apr 25;16(4):e59023. doi: 10.7759/cureus.59023. eCollection 2024 Apr. Cureus. 2024. PMID: 38803753 Free PMC article.
References
-
- Bournville. L’idiotie Mongolienne. Prog Med 1903;3:117
-
- Maranon G, Martinez D, Gochi Mendizabal JM. Mongolismeet macrogenitosomie. Ann Endocrinol 1951;12:41-8. - PubMed
-
- Fort P, Lifshitz F, Bellisario R, Davis J, Lanes R, Pugliese M, et al. Abnormalities of thyroid function in infants with Down syndrome. J Paediatr 1984;104:545-9. - PubMed
-
- Werder EA, Torresani T, Navratil F, Arbenz U, Eiholzer U, Pelet B, et al. Pericardial effusion as a sign of acquired hypothyroidism in children with Down syndrome. Eur J Pediatr 1993;52:397-8. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous