

Discordance between anatomical and functional coronary stenosis severity
- PMID: 17612701
- PMCID: PMC1847721
Discordance between anatomical and functional coronary stenosis severity
Abstract
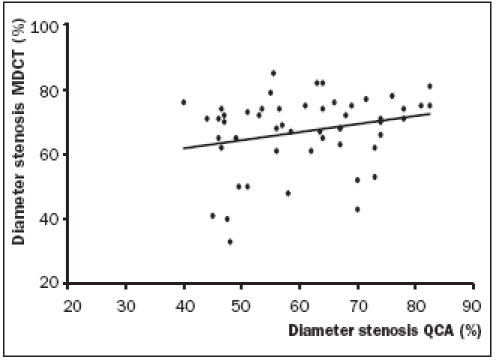
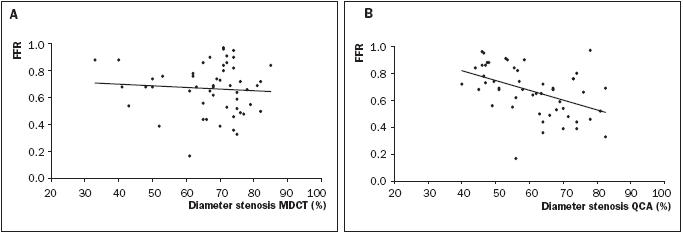
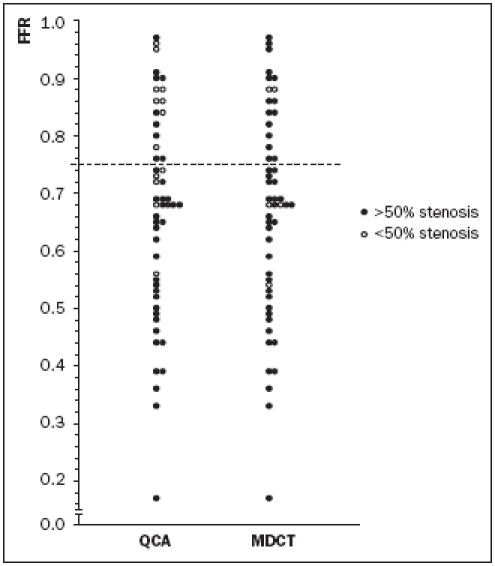
BACKGROUND.: New developments have made 16-slice multidetector computed tomography (MDCT) a promising technique for detecting significant coronary stenoses. At present, there is a paucity of data on the relation between fractional flow reserve (FFR) measurement and MDCT stenosis detection. OBJECTIVE.: The aim of this study was to investigate the relation between the anatomical severity of coronary artery disease detected by MDCT and functional severity measured by fractional flow reserve (FFR). METHODS.: We studied 53 patients (39 men and 14 women, age 62.5+/-8.1 years) with single-vessel disease scheduled for percutaneous coronary intervention (PCI). All patients underwent MDCT scanning one day prior to PCI and FFR was measured before PCI in the target vessel. RESULTS.: MDCT analysis could be performed in 52 of 53 patients (98.1%) and all patients had adequate FFR and quantitative coronary angiography (QCA) measurements. The mean stenosis diameters calculated by MDCT and QCA were 67.0+/-11.6% and 60.8+/-11.6% respectively. No significant relation was found between MDCT and QCA (r=0.22, p=0.12) The mean FFR in all patients was 0.67+/-0.18. A relation of r=-0.46 (p=0.0006) between QCA and FFR was found. In contrast, no relation between MDCT and FFR could be demonstrated (r=-0.09, p=0.50). Furthermore, a high incidence of false-positive and false-negative findings was present in both diagnostic modalities. CONCLUSION.: There is no clear relation between the anatomical and functional severity of coronary artery disease as defined by MDCT and FFR. Therefore, functional assessment of coronary artery disease remains mandatory for clinical decisionmaking. (Neth Heart J 2007;15:5-11.).
Figures
Similar articles
-
Comprehensive assessment of coronary artery stenoses: computed tomography coronary angiography versus conventional coronary angiography and correlation with fractional flow reserve in patients with stable angina.J Am Coll Cardiol. 2008 Aug 19;52(8):636-43. doi: 10.1016/j.jacc.2008.05.024. J Am Coll Cardiol. 2008. PMID: 18702967
-
Diagnostic performance of quantitative coronary computed tomography angiography and quantitative coronary angiography to predict hemodynamic significance of intermediate-grade stenoses.Int J Cardiovasc Imaging. 2015 Dec;31(8):1651-61. doi: 10.1007/s10554-015-0748-1. Epub 2015 Sep 1. Int J Cardiovasc Imaging. 2015. PMID: 26323355
-
Visual-functional mismatch and results of fractional flow reserve guided percutaneous coronary revascularization.J Med Assoc Thai. 2014 Oct;97(10):1064-76. J Med Assoc Thai. 2014. PMID: 25632623
-
CT Angiography for the Prediction of Hemodynamic Significance in Intermediate and Severe Lesions: Head-to-Head Comparison With Quantitative Coronary Angiography Using Fractional Flow Reserve as the Reference Standard.JACC Cardiovasc Imaging. 2016 May;9(5):559-64. doi: 10.1016/j.jcmg.2015.08.021. Epub 2016 Feb 17. JACC Cardiovasc Imaging. 2016. PMID: 26897669
-
Fractional flow reserve versus angiography guided percutaneous coronary intervention: An updated systematic review.Catheter Cardiovasc Interv. 2018 Jul;92(1):18-27. doi: 10.1002/ccd.27302. Epub 2017 Oct 5. Catheter Cardiovasc Interv. 2018. PMID: 28980386
Cited by
-
Triple rule-out CT coronary angiography: three of a kind?Int J Cardiovasc Imaging. 2009 Mar;25(3):327-30. doi: 10.1007/s10554-008-9381-6. Epub 2008 Nov 11. Int J Cardiovasc Imaging. 2009. PMID: 19002601 No abstract available.
-
Journal metrics for the Netherlands Heart Journal.Neth Heart J. 2011 Apr;19(4):159-161. doi: 10.1007/s12471-011-0099-z. Epub 2011 Mar 3. Neth Heart J. 2011. PMID: 21475678 Free PMC article. No abstract available.
-
Quantitative coronary arterial stenosis assessment by multidetector CT and invasive coronary angiography for identifying patients with myocardial perfusion abnormalities.J Nucl Cardiol. 2012 Oct;19(5):922-30. doi: 10.1007/s12350-012-9598-6. Epub 2012 Jul 20. J Nucl Cardiol. 2012. PMID: 22814771
-
Use of the anterior-posterior chest diameter in CT: reduction in radiation dose?Int J Cardiovasc Imaging. 2010 Dec;26(8):941-5. doi: 10.1007/s10554-010-9647-7. Epub 2010 Jun 5. Int J Cardiovasc Imaging. 2010. PMID: 20526742 Free PMC article. No abstract available.
-
Reduction of radiation dose using 80 kV tube voltage: a feasible strategy?Int J Cardiovasc Imaging. 2012 Feb;28(2):425-8. doi: 10.1007/s10554-011-9845-y. Epub 2011 Mar 19. Int J Cardiovasc Imaging. 2012. PMID: 21424152 Free PMC article. No abstract available.
References
-
- Fischer JJ, Samady H, McPherson JA, et al. Comparison between visual assessment and quantitative angiography versus fractional flow reserve for native coronary narrowings of moderate severity. Am J Cardiol 2002;90:210-5. - PubMed
-
- Kimball BP, Bui S, Cohen EA, Cheung PK, Lima V. Systematic bias in the reporting of angioplasty outcomes: accuracy of visual estimates of absolute lumen diameters. Can J Cardiol 1994;10: 815-20. - PubMed
-
- Reiber JH, van der Zwet PM, Koning G, et al. Accuracy and precision of quantitative digital coronary arteriography: observer-, short-, and medium-term variabilities. Cathet Cardiovasc Diagn 1993;28:187-98. - PubMed
-
- Topol EJ, Nissen SE. Our preoccupation with coronary luminology. The dissociation between clinical and angiographic findings in ischemic heart disease. Circulation 1995;92:2333-42. - PubMed
-
- Zijlstra F, Fioretti P, Reiber JH, Serruys PW. Which cineangiographically assessed anatomic variable correlates best with functional measurements of stenosis severity? A comparison of quantitative analysis of the coronary cineangiogram with measured coronary flow reserve and exercise/redistribution thallium-201 scintigraphy. J Am Coll Cardiol 1988;12:686-91. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous