

Procalcitonin guided antibiotic therapy and hospitalization in patients with lower respiratory tract infections: a prospective, multicenter, randomized controlled trial
- PMID: 17615073
- PMCID: PMC1947969
- DOI: 10.1186/1472-6963-7-102
Procalcitonin guided antibiotic therapy and hospitalization in patients with lower respiratory tract infections: a prospective, multicenter, randomized controlled trial
Abstract
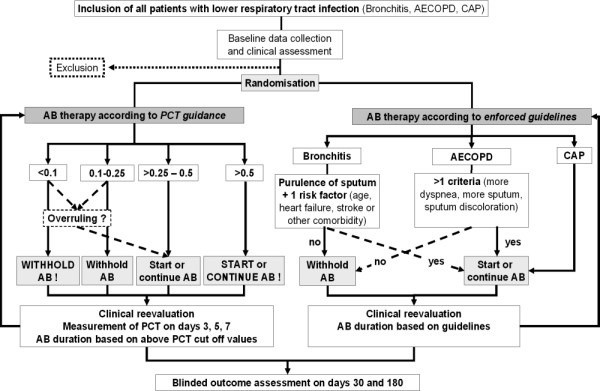
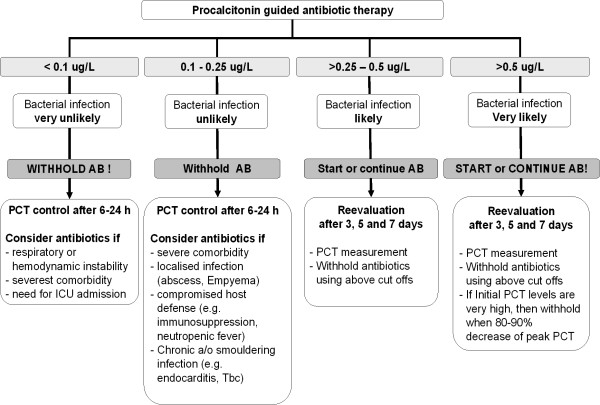
Background: Lower respiratory tract infections like acute bronchitis, exacerbated chronic obstructive pulmonary disease and community-acquired pneumonia are often unnecessarily treated with antibiotics, mainly because of physicians' difficulties to distinguish viral from bacterial cause and to estimate disease-severity. The goal of this trial is to compare medical outcomes, use of antibiotics and hospital resources in a strategy based on enforced evidence-based guidelines versus procalcitonin guided antibiotic therapy in patients with lower respiratory tract infections.
Methods and design: We describe a prospective randomized controlled non-inferiority trial with an open intervention. We aim to randomize over a fixed recruitment period of 18 months a minimal number of 1002 patients from 6 hospitals in Switzerland. Patients must be >18 years of age with a lower respiratory tract infections <28 days of duration. Patients with no informed consent, not fluent in German, a previous hospital stay within 14 days, severe immunosuppression or chronic infection, intravenous drug use or a terminal condition are excluded. Randomization to either guidelines-enforced management or procalcitonin-guided antibiotic therapy is stratified by centre and type of lower respiratory tract infections. During hospitalization, all patients are reassessed at days 3, 5, 7 and at the day of discharge. After 30 and 180 days, structured phone interviews by blinded medical students are conducted. Depending on the randomization allocation, initiation and discontinuation of antibiotics is encouraged or discouraged based on evidence-based guidelines or procalcitonin cut off ranges, respectively. The primary endpoint is the risk of combined disease-specific failure after 30 days. Secondary outcomes are antibiotic exposure, side effects from antibiotics, rate and duration of hospitalization, time to clinical stability, disease activity scores and cost effectiveness. The study hypothesis is that procalcitonin-guidance is non-inferior (i.e., at worst a 7.5% higher combined failure rate) to the management with enforced guidelines, but is associated with a reduced total antibiotic use and length of hospital stay.
Discussion: Use of and prolonged exposure to antibiotics in lower respiratory tract infections is high. The proposed trial investigates whether procalcitonin-guidance may safely reduce antibiotic consumption along with reductions in hospitalization costs and antibiotic resistance. It will additionally generate insights for improved prognostic assessment of patients with lower respiratory tract infections.
Trial registration: ISRCTN95122877.
Figures
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
