

The epidemiological and clinical characteristics of patients admitted for coronary angiography to evaluate ischemic heart disease
- PMID: 17616023
- PMCID: PMC2687617
- DOI: 10.3904/kjim.2007.22.2.87
The epidemiological and clinical characteristics of patients admitted for coronary angiography to evaluate ischemic heart disease
Abstract
Background: Most of the known risk factors associated with ischemic heart disease are based on studies from Western countries; there is only limited information on Korean populations. This study was designed to analyze age related differences in epidemiologic and clinical characteristics in patients who were admitted for coronary angiography for the evaluation of ischemic heart disease.
Methods: As part of the multicenter KCAR (Korean Coronary Artery disease Registry) Study, the clinical data of 6,549 patients, who were evaluated at the cardiac catheterization laboratory by coronary angiography, at seven university hospitals in Korea from March 1999 to December 2005, were registered into the KCAR database and analyzed. All patients were divided into three groups according to age: age < or = 40, age 41-70 and age > or = 71. All demographic and coronary angiographic features were analyzed for the different groups.
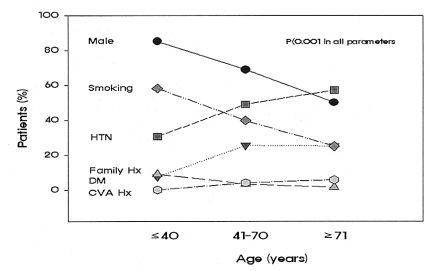
Results: The demographic data showed that compared to the older patients young patients < or = 40 had a higher prevalence of males and smokers, but a lower prevalence of hypertension, diabetes and prior history of stroke and myocardial infarction. For the lipid profiles, the younger patients had much higher levels of total cholesterol, triglycerides and LDL-cholesterol than the older groups; however, there was no difference in the HDL-cholesterol levels among the three age groups. The most common component of the metabolic syndrome was obesity (79%) in the younger patients and hypertension (92%) in the older patients. The most common reason for presentation was ST-segment elevated myocardial infarction in the younger patients and unstable angina in the older patients.
Conclusions: Ischemic heart disease in younger adults < or = 40 had different demographic characteristics and clinical presentation than older patients.
Figures




Similar articles
-
[Coronary risk factors and mode of ischemic heart disease treatment in patients over 65 years of age].Przegl Lek. 2003;60(7):451-5. Przegl Lek. 2003. PMID: 14750417 Polish.
-
Prevalence of diabetes and other cardiovascular risk factors in an Iranian population with acute coronary syndrome.Cardiovasc Diabetol. 2006 Jul 17;5:15. doi: 10.1186/1475-2840-5-15. Cardiovasc Diabetol. 2006. PMID: 16842631 Free PMC article.
-
[Changes in the prevalence of metabolic syndrome and smoking habits during a 10-year period and relation between these risk factors and ischemic heart disease among men aged 45-64 years].Medicina (Kaunas). 2008;44(5):400-6. Medicina (Kaunas). 2008. PMID: 18541957 Lithuanian.
-
API expert consensus document on management of ischemic heart disease.J Assoc Physicians India. 2006 Jun;54:469-80. J Assoc Physicians India. 2006. PMID: 16909697 Review.
-
Myocardial infarction in women.Epidemiol Rev. 1983;5:67-95. doi: 10.1093/oxfordjournals.epirev.a036265. Epidemiol Rev. 1983. PMID: 6357823 Review.
Cited by
-
Acute coronary syndrome in the young: clinical characteristics, risk factors and prognosis.Open Cardiovasc Med J. 2014 Jul 25;8:61-7. doi: 10.2174/1874192401408010061. eCollection 2014. Open Cardiovasc Med J. 2014. PMID: 25152777 Free PMC article.
-
Impact of smoking on clinical outcomes in female patients with acute myocardial infarction.Korean Circ J. 2015 Jan;45(1):22-7. doi: 10.4070/kcj.2015.45.1.22. Epub 2015 Jan 26. Korean Circ J. 2015. PMID: 25653700 Free PMC article.
-
Prediabetes and all-cause mortality in young patients undergoing coronary artery angiography: a multicenter cohort study in China.Cardiovasc Diabetol. 2023 Mar 1;22(1):42. doi: 10.1186/s12933-023-01776-w. Cardiovasc Diabetol. 2023. PMID: 36859269 Free PMC article.
-
Clinical significance of on-treatment triglyceride level in patients treated by percutaneous coronary intervention for non-ST-segment elevation acute coronary syndrome.Korean J Intern Med. 2009 Dec;24(4):330-6. doi: 10.3904/kjim.2009.24.4.330. Epub 2009 Nov 27. Korean J Intern Med. 2009. PMID: 19949731 Free PMC article.
References
-
- Yan RT, Yan AT, Tan M, Chow CM, Fitchett DH, Ervin FL, Cha JY, Langer A, Goodman SG. Age-related differences in the management and outcome of patients with acute coronary syndromes. Am Heart J. 2006;151:352–359. - PubMed
-
- Shiraishi J, Kohno Y, Yamaguchi S, Arihara M, Hadase M, Hyogo M, Yagi T, Shima T, Sawada T, Tatsumi T, Azuma A, Matsubara H. Medium-term prognosis of young Japanese adults having acute myocardial infarction. Circ J. 2006;70:518–524. - PubMed
-
- Katzel LI, Sorkin KD, Colman E, Goldberg AP, Busby-Whitehead MJ, Lakatta LE, Becker LC, Lakatta EG, Fleg JL. Risk factors for exercise-induced silent myocardial ischemia in healthy volunteers. Am J Cardiol. 1994;74:869–874. - PubMed
-
- Avendano M, Kunst AE, Huisman M, Lenthe FV, Bopp M, Regidor E, Glickman M, Costa G, Spadea T, Deboosere P, Borrell C, Valkonen T, Gisser R, Borgan JK, Gadeyne S, Mackenbach JP. Socioeconomic status and ischaemic heart disease mortality in 10 western European populations during the 1990s. Heart. 2006;92:461–467. - PMC - PubMed
-
- Chaturvedi S. The seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7): is it really practical? Natl Med J India. 2004;17:227. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials